










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkActa Médica Costarricense
On-line version ISSN 0001-6002Print version ISSN 0001-6012
Acta méd. costarric vol.63 n.2 San José Apr./Jun. 2021
Articles
Infant mortality due to congenital defects in Costa Rica: 2010-2018 update
1Instituto Costarricense de Investigación y Enseñanza en Nutrición y Salud (INCIENSA), Unidad de Enfermedades Congénitas (UEC), Centro de Registro de Enfermedades Congénitas (CREC). Tres Ríos, Cartago, Costa Rica.
About 3% to 5% of all newborns worldwide are born with a birth defect (CD).1 Its n with serious CD and 95% of deaths, largely due to high birth rates and limited access to prenatal diagnosis. 2
In the 1980s, in Latin America and the Caribbean, the proportion of infant deaths attributed to CD increased from 2% to 27% and, since then, they represent one of the 5 leading causes of death in the region (Health conditions in the Americas. Pan American Health Organization, 1986). In Latin American countries, where infant mortality has fallen below 50 per 1 000 births, the CD is the third leading cause of death, which makes it a significant public health problem.3
In the last decade, Costa Rica, a middleincome country, presented an annual average of 71 000 births (98% in-hospital) and an infant mortality rate (IMR) of 8.37 for the year 2018; CD accounted for 35% of the IMR, surpassed only by perinatal conditions (Annual bulletin. Instituto Nacional de Estadística y Censos Infant mortality and recent evolution 2018). The prevalence of CD in the last five years in Costa Rica ranged between 2.6-3.2 per 100 births (Annual birth defects report. Inciensa, 2019).
The IMR is an indicator of the living conditions and environment in which a nation develops. It is one of the best and most accessible indicators of the health of a population, synthesizing many of the components of health while being sensitive to both health interventions and general living conditions.4
The most marked reduction in the IMR in Costa Rica occurred in the 1970s and 1980s, mainly due to the decrease in infectious, immunopreventable, and parasitic diseases (Desigualdades de Salud en Costa Rica: Una aproximación geográfica - poblacional / Health Inequalities in Costa Rica: a geographicpopulation approach. PAHO, 2004). This phenomenon had a multifactorial origin, since it occurred in a context of great economic and social improvements, a notable drop in fertility, and a radical transformation of health programs and organization of the sector.5
While there are many studies analyzing infant mortality and its risk factors, the contribution of CD to IMR and neonatal mortality rate (NMR) has been much less explored.
The last analysis of the IMR for birth defects (IMBD) in Costa Rica has carried out with data from 1981 to 2010.6 This report identified a significant reduction in IMR in the nervous, digestive and circulatory system CD groups; except for the circulatory system, these groups experienced a significant drop in their NMR. However, an analysis of specific congenital defects was not performed, but only by the system, leaving the question as to which specific DC has the greatest weight in the IMBD.
In the last decade, events related to CD have occurred that could have affected IMBD. One of them has been the management adopted since 2014 by the Hospital Nacional de Niños as a national reference center for diagnosis and cardiac surgery in children, to improve surgical interventions in children with congenital heart disease (Caja Costarricense de Seguro Social, 2016. https:// www.ccss.sa.cr/noticia?logros-espectaculares-encirugia- cardiaca-pediatrica). Another event was the zika virus emergency in the country in 2016, with a corresponding increase in some central nervous system defects, such as microcephaly (Abbreviated report of microcephaly cases reported to CREC, Costa Rica, 2011-2017). In this context, South American countries such as Brazil, demonstrated a 5% increase in IMR in 2016 compared to 2015, attributed according to health authorities to the zika virus epidemic and the economic crisis.7
This study aimed to identify the trend of the different types of congenital defects in IMT and NTM in Costa Rica from the period 2010 to 2018 and to perform a comparative analysis with the period 2000 to 2009.
Methods
An analysis of vital statistics was conducted.
The source of information was the Instituto Nacional de Estadísticas y Censos de Costa Rica (INEC) through its online consultation system (https://www.inec.cr/sistema-de-consultas) for demographic statistics with public access. The base of deaths by specific cause and the base of births for the period 2010-2018 was consulted. In addition, although both the IMRBD and the neonatal mortality rate due to congenital defects (NDMR) had already been analyzed in a publication,6 the same databases were consulted to obtain the estimates for the period 2000-2009, to compare them with the new period to be analyzed 2010-2018 and adjust the trend according to period, for congenital anomalies in general and by specific CD. This last analysis was not done in the previously mentioned report, as it provided estimates only by large groups of CD.
Details of the causes by CD of neonatal deaths were obtained from the tables prepared for this purpose by INEC each year1 , which are classified according to the Manual of the International Statistical Classification of Diseases, Injuries, and Causes of Death in its tenth edition.
The IMBD and IMBD rates year were calculated, as well as their trend in the period 2000-2018. In addition, the weight of infant and neonatal deaths due to CD in the overall IMR was calculated.
The following groups of congenital defects were analyzed: nervous system (Q000-Q079), circulatory system (Q200-Q289), respiratory system (Q300-Q349), digestive system (Q380-Q459), urinary system (Q600-Q649), musculoskeletal system (Q650-Q799), other syndromes and congenital anomalies (Q860-Q899), chromosomal anomalies (Q900-Q999) and finally skin, face, neck, and genital DC were grouped (Q800-Q859, Q100-Q189, Q350-Q379, Q500-Q564).
The main specific causes of infant and neonatal death by CD were identified and the defects with the highest number of deaths during the 19 years of analysis were selected.
For trend analysis, a linear Poisson Log regression model was constructed (module: generalized linear models, software: SPSS. Statistics) adjusted by period, taking as a base the period 2000-2009, not only for each CD group but also for the main specific causes of infant mortality by CD. The model used is represented as follows:
Log (mortality rate) = β0 + β1 × (period of time)
From this model, marginal means were obtained for the IMBD and IMBD rates, as well as the prevalence ratios (PR) corresponding to the periods with their respective confidence intervals (95%CI). These results were compared using the Wald chi-square tests. The significance level used was 0.05.
The results were grouped in two tables and one figure. Table 2 shows the CDs with more than 50 deaths during the period analyzed.
This report corresponds to an analysis of publicly available vital statistics and was approved by the Research Directorate of the Costa Rican Institute for Research and Education in Nutrition and Health (INCIENSA).
Results
In Costa Rica, the trend of the overall IMR in the last 19 years (2000-2018) has been downward, ranging between 11.1 and 7.7 per 1,000 births. However, the NMR, which occupies about 71% of the IMR, has presented a much more discrete decline, ranging between 7.6 and 5.9 per 1000 births. CD accounted f or 33.6% of infant mortality during these almost two decades, while neonatal deaths due to CD accounted for 32% of total neonatal deaths. The NIDDMR ranged between 2.5 and 3.7 per 1000 births, showing a decrease; while the NIDDMR ranged between 1.8 and 2.4 per 1000 births, but its behavior was practically flat (Figure 1).
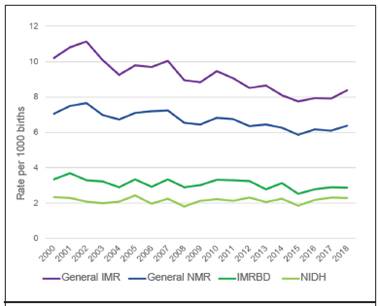
Figure 1 The trend in overall infant mortality rate (IMR) and neonatal mortality rate (NMR) and infant and neonatal mortality rates for congenital defects (IMRBD and NIDH). Costa Rica, 2000-2018.
To analyze the significance of these changes, a period-adjusted Poisson regression was performed, comparing the period 2010-2018 versus 2000-2009.
In the 2010-2018 period, the overall IMR was 8.42 per thousand (95% CI: 8.2-8.65) and presented a significant decrease from the previous decade (9.88 per thousand, 95% CI: 9.7-10). The IMRDMR also presented a significant decrease of 7% in the period 2010-2018 (Table 1), going from 3.19 to 2.97 per thousand; however, as the decrease in the overall IMR was greater than the decrease in the IMRDMR, the percentage contributed by CD in the IMR in the last decade is higher going from 32.25% in the period 2000-2009 to 35.43%. Concerning the overall NMR, there was also a significant decrease from 7.04 (95%CI 6.8-7.2) to 6.34 per thousand (95%CI 6.2- 6.5); however, there was no significant change in the NCMR, which went from 2.13 to 2.17 per thousand, or in the percentage weight of CD in the NMR.
When analyzing the different CD groups separately, we see that the decrease in the IMBD was mainly at the expense of the circulatory and digestive systems. In all the other CD groups, the difference was not significant or there was even an increase, the latter being significant only in the respiratory system (Table 1).
About the NCMDD, an increase of 2% was observed in the periods analyzed, but this change was not statistically significant. Only the circulatory system, 99.8% of whose defects correspond to congenital heart disease, showed a significant decrease of 25%, while the other systems showed no significant changes or an increase, as was the case with the respiratory system and chromosomopathies (Table 1).
Table 1 Infant and neonatal mortality according to birth defects (CD) groups and prevalence ratio, for the period 2010-2018, based on the period 2000-2009.

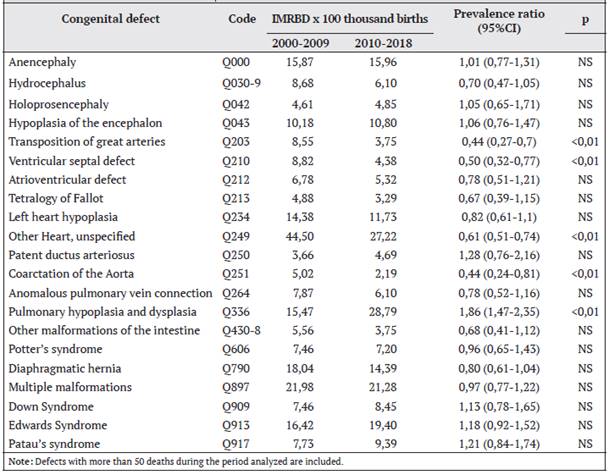
Table 2 shows the change in IMR according to specific CD; a significant decrease in causality was identified for some cardiac defects such as transposition of the great arteries, ventricular septal defect, coarctation of the aorta, and other unspecified cardiac anomalies. Some other DC that presented significant changes does not appear, because the number of deaths was less than 50 as the established limit. However, among the latter, spina bifida presented a significant decrease in IMR (p <0.05) from 2.58 to 1.10 per 100 thousand births (PR: 0.42; a decrease of 58%); while other CD presented a significant increase (p <0.01) in their MR, such as gastroschisis that went from 1.36 to 4.69 x 100 thousand births (PR: 3.46; increase of 246%), Siamese twins from 0.41 to 2.82 x 100 thousand births (PR: 6.92; increase of 592%) and code Q870-8 corresponding to “other specified syndromes” whose IMR increased from 2.04 to 5.16 x 100 thousand births (PR: 2.54; an increase of 154%). Pulmonary hypoplasia and dysplasia also showed a significant increase (Table 2).
Table 2 Infant mortality rate due to congenital defect (IMRBD) and prevalence ratio, for the period 2010-2018, based on the period 2000-2009.
Regarding the NMR by specific CD, a significant decrease (p<0.01) was identified in only two cardiac defects: transposition of the great arteries, which went from 5.16 to 2.35 per 100 000 (PR: 0.46; 54% decrease) and other unspecified cardiac anomalies, which went from 27.68 to 15.18 per 100 000 (PR: 0.55; 45% decrease). This last group (unspecified cardiac anomalies) corresponds to a series of congenital heart diseases that were not defined at the time of filling out the death certificate, either because they had not been diagnosed at the time of death registration or because the diagnosis was not correctly noted.
The same specific DCs that showed significant increases in IMR did so in NMR: gastroschisis which went from 1.22 to 3.75 x 100 thousand births (PR: 3.08; 208% increase), pulmonary hypoplasia and dysplasia which rose from 10.85 to 22.06 x 100 thousand births (PR: 2.03; 103% increase); Siamese twins, from 0.41 to 2.82 x 100 thousand births (PR: 6.92; 592% increase); and other specified syndromes, from 0.68 to 2.66 x 100 thousand births (PR: 3.92; 292% increase).
In general, the digestive system showed a significant decrease in infant mortality, but not in neonatal mortality. However, when disaggregating the main digestive anomalies as a cause of death, although there was a decrease in all of them, none of them was significant.
Discussion
By identifying the trend of the different types of birth defects in IMR and NTMR in the country during the period 2010-2018 and performing a comparative analysis with the period 2000-2009, it was found that, in Costa Rica, previous analyses showed a significant decrease in both IHMR and NSTEMI from 1981 to 2010.6 With this work, a significant decrease in both IMR and NTMR was documented between 2010-2018 concerning the previous decade. Likewise, a significant decrease of 7% was documented in the IHMR, even though the NCMR did not show significant changes.
Around the world, despite advances in the reduction of IMR, the decrease in U5MR has not been as relevant.8 Thus, CD constitutes one of the great challenges for health agendas worldwide and particularly in the Americas region, whereby in 2017, 15 out of every thousand births were at risk of dying during the first year of life and 10 out of every thousand during the first month (United Nations Inter-agency Group of Child Mortality Estimation. Levels and trends in child mortality: report 2018. United Nations Children’s Fund, 2018).
In Latin America, approximately one in five neonatal deaths in the region is due to CD; moreover, the proportion of neonatal deaths due to CD has increased from 16.2% to 22.3% between 2000 and 2016, an increase that is notable in most countries worldwide.
A recent analysis by the Pan American Health Organization (Present and Future of Birth Defects Surveillance in the Americas. PAHO-World Bank, 2019) it was determined that in countries where the NIMR is less than 6 per 1000 births, CD deaths represent 15%-40% of the total; those with a NIMR between 6 to 12 per 1000 births, the percentage weight fluctuates between 10%-30%; while, for those countries where the NIMR is higher than 12 per 1000, CD deaths generally represent less than 15% of the total in that age group. Referring to the results of this analysis, in Costa Rica, where the NIMR is 6.34 per 1000, neonatal deaths due to CD accounted for 32% of overall neonatal mortality. Also, at the national level, the NCMR for the period studied represented 73% of the IDDMR; and it has been reported that, in developed countries, 70% of deaths due to congenital anomalies occur in the neonatal period.9
Contrary to what has happened in our country, some Latin American countries have shown an increase in the IMR in recent decades. 10,11 In Mexico, for example, the IMR decreased by more than 57% between 1990 and 2012; however, infant deaths due to CD remained stable, with a slight upward trend, so their relative weight increased from 13.7% to 33.8%.12 In Brazil, during the period 1996-2010, there was an increase in both the U5MR and the percentage of deaths due to CD.13
On the other hand, similar to our country, in the United States, a country where CD occupies the first place as a cause of infant mortality,14,15 the IMRBD has been decreasing since 1970, during the period 2003-2017 it decreased by 10% overall.16 According to the authors, the decrease in the IMRBD could have been influenced by improvements in prenatal care, prevention measures, and improvements in medical care, in addition to factors influencing overall infant mortality.
In Costa Rica, congenital heart disease is the most frequent CD and is the leading cause of infant mortality due to CD.17 According to our analysis, IMR and NMR for this cause decreased by 27 and 25% respectively from 2010 to 2018 compared to the previous decade. Thus, being a group of CD that is serious as well as frequent, a significant decrease in their mortality greatly impacts the IMRBD and NMRCD. This is what happened in our country; the decrease in the IMRBD was mainly due to a significant decrease in infant and neonatal mortality in cardiac defects. This is the first time in our country that a significant decrease in neonatal mortality for these reasons is evidenced, a phenomenon that requires further analysis to find out which factors contribute to this important improvement.
With IMR and NMR for nervous system defects in general, there was no significant change between the periods analyzed, nor was there a change for CD associated with congenital Zika (microcephaly, hypoplasia of the encephalon, hydrocephalus).
However, there was a significant decrease in infant mortality due to spina bifida, a fact already documented in the country and with the main decrease in IMR due to neural tube defects after 1997, mainly as a consequence of food fortification with folic acid.18
The only system that presented an increase in IMR was the respiratory system. However, it is important to clarify that 88% of the anomalies correspond to pulmonary hypoplasia and dysplasia (Q336), a possibly misclassified cause of death, which could be more related to a complication of prematurity than to a congenital defect. Similar results have been found in other analyses and suggest that this trend could be due to an increase in the misuse of this diagnosis.19
Chromosomal anomalies as a whole showed a significant increase in neonatal mortality.
However, when we disaggregated the main anomalies, although there was an increase in the NMR of each of the main chromosomal syndromes (Down syndrome, Edwards syndrome, and Patau syndrome), none of them was significant. If we take into account the prevalence at birth with data from the Centro de Registro de Enfermedades Congenitas at the national level, we find that there has been an increase in recent years for Edwards syndrome and Down syndrome20, which directly affects the increase in infant deaths from these causes.
IMR and NMR due to gastroschisis presented a significant increase in the last decade. This is probably due to the increase in their prevalence, which has been described both in Costa Rica and worldwide.21 Similarly, the group called Other specified syndromes (Q870-878), such as Siamese twins (Q894), presented a significant increase in rates. This could be due to an improvement in clinical diagnosis and therefore an increase in the number of cases, but it is a hypothesis that should be explored to determine whether the increase is due to an increase in registration as a cause of death, an increase in prevalence or mortality.
It is important to clarify that like all analyses of vital statistics, the findings are limited by the accuracy of the demographic and cause-ofdeath data included on child death certificates. However, vital statistics derived from national vital registration systems is an optimal source of mortality, fertility, and cause-of-death data because they are intended to cover the entire population, are available for subnational populations, and, in principle, result from a medically certified cause of each death.22 However, in the cause-specific analysis, we see limitations arising from a lack of diagnostic specificity, for example, the group of nonspecific cardiac anomalies, which ranks second in the IMRBD.
Finally, from the findings of this analysis, it can be concluded that the downward trend in the IMRBD in Costa Rica is similar to that found in developed countries, as well as the difficulty in significantly reducing the NMRBD; and that the significant decrease in the IMRBD is due to a significant decrease in IMR and NMR due to congenital heart disease, which is the most prevalent CD in the country. Prevention measures and improvements in timely prenatal medical care and care of newborns with CD should be strengthened to contribute to a further decrease in IMR and NMR due to this cause.
Abbreviations:
CD, congenital defect; INEC, Instituto Nacional de Estadística y Censo de Costa Rica; IMR, infant mortality rate; IMBD, infant mortality rate due to congenital defects; NMR, neonatal mortality rate; NDMR, the neonatal mortality rate due to congenital defects; PR, prevalence ratio. Support sources: none. Conflict of interest: none to declare. mbarboza@inciensa.sa.cr
Referencias
1. Kirby RS. The prevalence of selected major birth defects in the United States. Semin Perinatol. 2017;41:338-44. [ Links ]
2. Toobaie A, Yousef Y, Balvardi S, St-Louis E, Baird R, Guadagno E et al. Incidence and prevalence of congenital anomalies in low-and middle-income countries: a systematic review. J Pediatr Surg. 2019; 54:1089-93. [ Links ]
3. García H, Salguero GA, Moreno J, Arteaga C, Giraldo A. Frecuencia de anomalías congénitas en el Instituto Materno Infantil de Bogotá. Biomédica 2003; 23:161-72. [ Links ]
4. Gonzalez RM, Gilleskie D. Infant Mortality Rate as a Measure of a Country’s Health: A Robust Method to Improve Reliability and Comparability. Demography. 2017;54:701-20. [ Links ]
5. Rosero L. Determinantes del descenso de la mortalidad infantil en Costa Rica. Bol Of Sanit Panam. 1985;99:510-26. [ Links ]
6. Barboza-Arguello MP, Benavides-Lara A, Umaña L, Vargas-Leitón B. Mortalidad infantil por defectos congénitos en Costa Rica, 1981-2010. Rev Panam Salud Publica. 2013;34:304-11. [ Links ]
7. Colluci C. Brazil’s child and maternal mortality have increased against background of public spending cuts. BMJ. 2018; 362: k3583. doi:10.1136/bmj.k3583 [ Links ]
8. Lehtonen L, Gimeno A, Parra-Llorca A, Vento M. Early neonatal death: A challenge worldwide. Semin Fetal Neonatal Med. 2017;22:153-60. [ Links ]
9. Sarasqueta, P. Mortalidad infantil por malformaciones congénitas y prematurez en la Argentina: análisis de los criterios de reducibilidad. Arch Argent Pediatr. 2006;104:153-8. [ Links ]
10. Gómez-Alcalá AV, Rascón-Pacheco RA. La mortalidad infantil por malformaciones congénitas en México: un problema de oportunidad y acceso al tratamiento. Rev Panam Salud Publica. 2008;24:297-303. [ Links ]
11. Hernandez-Trejo M, Llano-Rivas I, Rivera A, Aguinaga-Ríos M, Mayen-Molina D. Mortalidad perinatal por defectos estructurales congénitos: un estudio de caso. Perinatol Reprod Hum. 2007;21:125-31. [ Links ]
12. Cantón SBF, Martínez AMH, Uribe RV. Mortalidad en menores de un año de edad por malformaciones congénitas del sistema nervioso central. México, 1990-2012. Bol Med Hosp Infant Mex. 2013;70:412-6. [ Links ]
13. Bronberg R, Schuler-Faccini L, Ramallo V, Alfaro M, Diperri J. Spatial and temporal analysis of infant mortality from congenital malformations in Brazil (1996-2010). J Community Genet. 2014;5:269-82. [ Links ]
14. Petrini J, Damus KY, Johnston R. An overview of infant mortality and birth defects in the United States. Teratology. 1997;56:8-9. [ Links ]
15. Petrini J, Dannus K, Rusell R. Contributionof birth defects to infant mortality in the United States. Teratology. 2002;66:3-6. [ Links ]
16. Almli LM, Ely DM, Ailes EC, Abouk R, Grosse SD, Isenburg JL, et al. Infant Mortality Attributable to Birth Defects - United States, 2003-2017. MMWR Morb Mortal Wkly Rep. 2020;69:25-9. [ Links ]
17. Benavides-Lara A, Faerron, JE, Umaña L, Romero-Zuñiga JJ. Epidemiología y registro de las cardiopatías congénitas en Costa Rica. Rev Panam Salud Publica. 2011;30:31-8. [ Links ]
18. Barboza MP, Umaña L. Impacto de la fortificación con ácido-fólico en los defectos del tubo neural en Costa Rica. Rev Panam Salud Pública. 2011;30:1-6. [ Links ]
19. Petrini J, Damus K, Jonston RB. Trends in infant mortality attributable to birth defects - United States, 1980-1995. MMWR Morb Mortal Wkly Rep. 1998;47:773-8. [ Links ]
20. Benavides-Lara A, Barboza-Argüello MP. Prevalencia al nacimiento de síndrome de Down, según edad materna en Costa Rica, 1996- 2016. Acta Med Costarric. 2019;61:177-82. [ Links ]
21. Barboza-Argüello MP, Benavides-Lara A. Prevalencia al nacimiento de gastrosquisis y onfalocele en Costa Rica. Acta Med Costarric. 2018;60:35-41. [ Links ]
22. Phillips DE, Lozano R, Naghavi M, Atkinson C, Gonzalez-Medina D, Mikkelsen L, et al. A composite metric for assessing data on mortality and causes of death: the vital statistics performance index. Popul Health Metrics. 2014;12:14. [ Links ]
Received: November 20, 2020; Accepted: July 12, 2021
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
