Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkHerpes zoster (HZ), also known as shingles or zoster, is a manifestation of the reactivation of the varicella-zoster virus (VZV), which, as a primary infection, induces chickenpox.
Following the initial VZV infection, the virus remains latent in sensory ganglia. In some individuals, latent VZV reactivates and replicates, perhaps as a consequence of waning cellular immunity, resulting in HZ.1,2 The blistering rash is the most distinctive feature of HZ, though the most frequently debilitating symptom is pain.3 The most significant clinical manifestations of HZ are acute neuritis and, later, post herpetic neuralgia (PHN),3 which frequently results in disordered sleep, chronic fatigue, anxiety and severe depression. Recent data indicate that the quality of life (QoL) and functional capacity of elderly persons can be severely affected by HZ to a degree that is comparable to such debilitating diseases as congestive heart failure, recent acute myocardial infarction, type II diabetes mellitus and clinical depression.4
Prevention and treatment for HZ and PHN present a significant unmet need. The zoster vaccine, Zostavax®, is a lyophilized preparation of the Oka/Merck strain of live attenuated VZV.5 Despite the proven successful vaccination prophylaxis shown to diminish the burden of illness due to HZ by 61%, HZ may still develop in a subset of patients.6
Early initiation of treatment with an antiviral agent has been shown to reduce the severity of acute HZ, as defined by the time to HZ rash healing and the duration of HZ-associated pain.
However, antiviral therapy has not consistently shown benefits in the treatment of PHN; data suggest that antiviral therapy has limited impact on the incidence of PHN, though it may shorten the duration of PHN pain.7 The role of corticosteroids has been evaluated in well-designed studies that demonstrate a modest effect on the acute phase of HZ, though no reduction has been observed in the frequency or severity of PHN following steroid monotherapy or combination therapy with antiviral drugs.2,8
HZ prevalence has been reported to affect 25 to 30% of the general population, though this rate rises above 50% among patients above 80 years old.9-12 The worldwide incidence of HZ is estimated between 1.2 to 3.4 cases per 1,000 healthy individuals per year though higher rates of 3.9 to 11.8 cases per 1,000 persons per year are reported by those aged above 65 years of age.13,14 However, it is commonly believed that geographic characteristics influence HZ development leading to differing HZ incidence rates between nations.15,16
The HZ epidemiology has not been reported in Costa Rica to our knowledge nor does the nation’s health authority collect this data. Nonetheless, Costa Rican hospital discharge data show that 63 cases of HZ required hospitalization in 2014 though this figure steadily declined from 152 HZ hospitalizations in 2000.17 Currently, there is no published data concerning HZ clinical characteristics, disease severity and health care resource utilization (HCRU) in patients from Costa Rica. Given the aging population of Costa Rica, the burden of HZ is expected to increase in coming years. The objective of this study was to measure the HZ-associated burden of illness, in terms of pain, impact on QoL and HCRU in a Costa Rican convenient sample from a single geriatric practice.
Materials and Methods
Study Design
This study is part of an international HZ study entitled MASTER (Monitoring and Assessing Shingles Through Education and Research) conducted in 8 countries in America and Asia aimed to evaluate the burden of illness associated with HZ and zoster-associated pain (ZAP).18-23 This was an observational prospective cohort and prevalence study of patients presenting with ZAP which included acute pain during zoster and PHN from the office of one geriatrician in Costa Rica.
The cohort was prevalent, as patients were recruited at various stages of their zoster episode, and prospective, as they were followed for 6 months thereafter.
The investigator obtained review board approval in compliance with local law. The study was conducted in accordance with the International Conference on Harmonization
Guidelines for Good Clinical Practices and the tenets of the Declaration of Helsinki. Eligible patients who provided written informed consent prior to participation were included in the study.
Study Population
Subjects were recruited prospectively between November 2008 and June 2010 and entered in the cohort at the time of presentation with zoster rash or ZAP symptoms.
Incident cases were defined as subjects recruited at the investigator’s office for a current zoster episode which had a duration of equal or less than 7 days. Prevalent cases were defined as patients enrolled while visiting the investigator for a current zoster episode which lasted longer than 7 days and for which the onset of rash had been recorded in the medical records. The onset of disease was defined by the zoster rash onset date rather than the date of cohort entry.
Patients who fulfilled all inclusion criteria and consented were eligible for study entry. Patients were required to be at least 50 years of age at the onset date of zoster rash and had a physicianconfirmed diagnosis of zoster rash or ZAP including acute pain or PHN. The date of onset was required to be documented in the patient’s chart. Patients were further expected to be capable of completing the study questionnaires, understanding the study and the content of the consent form, were in agreement to participate in the study by signing the informed consent and were available for the study follow-up period.
Study Schedule
Following the baseline assessment (day 0) conducted at the investigator’s office, nine assessments were conducted with the aid of self-administered questionnaires at days 7, 14, 21, 30, 60, 90, 120, 150 and 180 following the subjects’ cohort entry. Scheduled visits occurred at days 14, 30 and 180. All patients were followed for six months under the same schedule regardless of the phase of the disease at the time of enrollment.
Data was collected using case report forms (CRFs) and questionnaires. CRFs were completed at the physician’s office during the baseline visit. Questionnaires were completed by the patients and returned to the study physician or coordinator to be subsequently mailed to the data management and analysis centre in Canada.
Outcome Measures
The primary outcome assessed the burden of illness due to ZAP from HZ rash onset as measured by the Zoster Brief Pain Inventory (ZBPI) and the Initial Zoster Impact Questionnaire (IZIQ), the latter representing an extension of the ZBPI to assess prodromal pain.24 Impact of zoster and/or ZAP on QoL were measured with the Euro-QoL (EQ-5D) index 25 using Latin American weights 26. The EQ-5D was administered on two occasions to capture the patient’s usual QoL without zoster, ZAP or PHN as well as the QoL in his/her current health state.
Patient-reported HCRU was assessed via a simple questionnaire that was administered at each follow-up visit.
The questionnaire was used to record the visits to physicians or clinics, hospitalizations, use of other health related services including physiotherapy, nursing services, psychologists, rehabilitation, natural or alternative medicine, prescription medications, over the counter medications as well as diagnostic tests and procedures performed for the current episode.
Statistical Analysis
Descriptive statistics were produced for all variables of the study. Measures of central tendency (mean) and dispersion (standard deviation - SD) were produced for all continuous scale variables and frequency distributions for all categorical scale variables. The change in QoL over time from baseline after HZ rash appeared was assessed for statistical significance with the paired-samples t-test.
All statistical analyses were performed using the Statistical Package for Social Sciences (SPSS Inc., version 21, Chicago, IL, USA).
Results
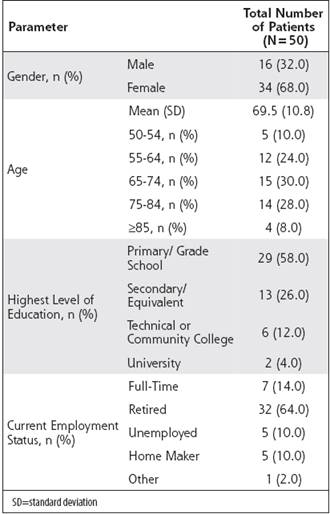
Table 1 presents the sample’s baseline characteristics including socio-demographics. A total of 50 patients were enrolled in the study including 46 (92.0%) and 4 (8.0%) prevalent and incident cases, respectively. Overall, 42 (84.0%), 42 (84.0%), 40 (80.0%), 39 (78.0%), 34 (68.0%), 31 (62.0%), 28 (56.0%), 28 (56.0%) and 27 (54.0%) completed the followup visits at day 7, 14, 21, 30, 60, 90, 120, 150 and 180, respectively. The majority of patients were female (68.0%) and retired (64.0%). The most common level of education at baseline was primary school (58.0%) followed by secondary school (26.0%). The baseline mean (SD) age was 69.5 (10.8) years.
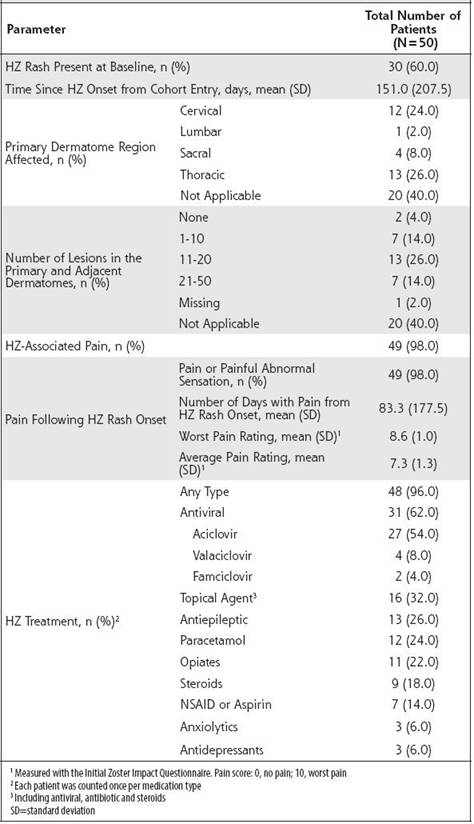
As presented in Table 2, 60.0% of patients presented with a HZ rash at baseline. The mean (SD) time since HZ onset duration was of 151.0 (207.5) days. The most frequently affected primary dermatome region was the thoracic region (26.0%) followed by the cervical (24.0%), sacral (8.0%) and lumbar (2.0%) regions. Following rash onset, 98.0% of patients experienced HZ-associated pain which persisted for a mean (SD) of 83.3 (177.5) days. PHN, defined as worst pain ≥3 after ≥90 days since rash onset, was experienced by 40 (80.0%) patients. The mean (SD) IZIQ worst and average pain ratings after rash onset were 8.6 (1.0) and 7.3 (1.3), respectively. The vast majority (96.0%) of patients had initiated HZ prescribed medications; the drugs most frequently administered were oral antivirals (62.0%), topical agents (32.0%), antiepileptic medications (26.0%), paracetamol (24.0%) and opiates (22.0%). (Table 2)
Figure 1 shows the worst and average ZAP levels in the last 24 hours over time. The mean (SD) worst ZBPI pain scores steadily decreased from 7.7 (1.8) at baseline to 5.9 (2.7) at day 180. Similarly, the mean (SD) average ZBPI pain scores decreased from 6.6 (1.7) at baseline to 4.0 (2.2) at day 180.
Figure 2 presents the QoL over time before and after HZ episode as measured by the Latin EuroQoL (EQ-5D) Index scores. The EQ-5D score was highest at baseline prior to HZ episode with a mean (SD) score of 0.8 (0.2). The EQ-5D scores decreased after rash onset at baseline with a mean (SD) of 0.4 (0.2) and increased to 0.7 (0.1) at day 180, indicating an improvement of QoL over time though without full QoL base recovery. Statistically significant differences (p<0.05) were observed between baseline EQ-5D index scores prior to rash onset and all follow-up visits (Figure 2).
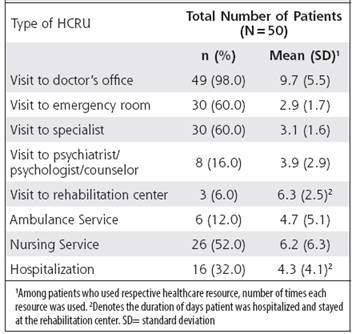
Table 3 shows the HCRU during the observation period including the proportions of patients requiring health resources as well as the mean time or duration of days associated with each resource use. Outpatient physicians were the most consulted healthcare professional with 98.0% of patients visiting their doctor, followed by visits to a specialist (60.0%), emergency room (60.0%), nursing services (52.0%), hospitalizations (32.0%), and psychiatrists (16.0%). Among patients who used the respective healthcare resource, the highest mean (SD) was observed for visits to the doctor’s office with 9.7 (5.5) times, rehabilitation center with 6.3 (2.5) days, and nursing services with 6.2 (6.3) times.
Discussion
This study aimed to assess the burden of illness, the impact on quality of life, and the HCRU associated with HZ in a single geriatric practice in Costa Rica. To our knowledge, this is the first study prospectively assessing the HZ burden of illness in Costa Rica. Overall, significant HZ-associated pain was observed during the course of the study after HZ rash onset which was associated with decreased QoL and increased HCRU. As ageassociated immune deficiency (immunosenescence) is known to increase the risk of HZ development 21,22, HZ prevention and management represents an important challenge to overcome particularly as 15.9% of the Costa Rican population was aged above 55 years in 2015 as per the World Factbook of the Central Intelligence Agency.
At study baseline, nearly all patients experienced HZassociated pain (98%). The worst pain, as measured by the ZBPI in the last 24 hours, was experienced immediately following rash onset and improved in the first 14 days of the observation period though slightly increased up to day 180. As a result, EQ-5D scores indicated an initial worsening of QoL following rash onset followed by a gradual improvement up to day 180.
Despite a slight amelioration of QoL during the observation period, EQ-5D levels did not return to pre-HZ episode values at day 180. Statistically significant differences (p<0.05) were observed between pre-HZ rash EQ-5D index scores and all follow-up visits. The persistence of pain and of low QoL illustrate the long recovery period associated with HZ and its significant burden of illness.
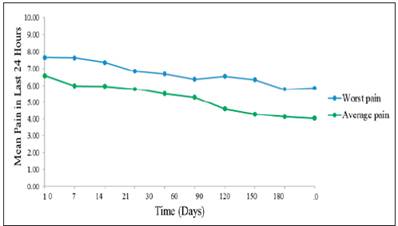
Figure 1 Mean HZ-Associated Worst pain and Average Pain, as measured by ZBPI, in the last 24 hours over Time
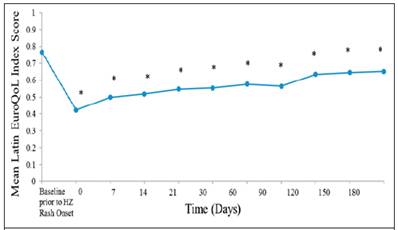
Figure 2. Mean Quality of Life EQ-5D Index Score using Latin American Weights over Time P-value assessed change in EQ-5D between baseline prior to HZ rash onset and day 0 to day 180 with the paired samples t-test. *Denotes statistical significance: day 0 (p<0.001); day 7 (p<0.001); day 14 (p<0.001); day 21 (p<0.001); day 30 (p<0.001); day 60 (p=0.003); day 90 (p<0.001); day 120 (p=0.004); day 150 (p<0.001); day 180 (p<0.001).
In accordance with severe burden of illness, significant HCRU was associated with HZ management as observed over the 180-day period, including visits to the doctor’s office (98%), emergency room (60%), specialists (60%), nursing services (52%), and hospitalizations (32%). The high burden associated with HZ is further illustrated in additional studies by the high HZ management costs.27
In terms of medications, aciclovir was the most frequently prescribed HZ medication (54.0%). This could be due to the fact that aciclovir, but not famciclovir and valaciclovir, is included in the drug formulary of the national social security system (Caja Costarricense de Seguro Social). Alternatively, physician preference may have further impacted medication prescription, particularly as only one investigator recruited patients in the current study.
These results should be interpreted in consideration of the study limitations. The study population included older patients (>50 years) seeking care for HZ which probably includes more severe cases of HZ compared to the general population and were recruited through a single private geriatric practice which further increases the likelihood of selection bias. The use of patient questionnaires carries the risk of variability among patients as pain is a subjective outcome. Their use is further associated with the risk of recall bias, particularly among prevalent cases for whom a time lag existed between HZ onset and inclusion in the study. The outcome of HZ may have been misclassified as no laboratory test was performed to confirm the presence of HZ. Furthermore, the inclusion of merely one study investigator and of a small patient sample may not be representative of the Costa Rican HZ population limiting the generalizability of the results; however, overall, the results of the current study are comparable to global estimates as reported by Kawai et al.28
Overall, this study has shown that severe morbidity, compromised quality of life, and significant healthcare utilization was associated with HZ among elders in Costa Rica. These results support the need for early intervention and preventive strategies, one of such could be the implementation of a HZ vaccination program, to reduce the HZ-associated disease burden in Costa Rica.
Acknowledgments and Collaborators: Not applicable