










Servicios Personalizados
Revista
Articulo
 texto en
texto en  Español (pdf)
Español (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkActa Médica Costarricense
versión On-line ISSN 0001-6002versión impresa ISSN 0001-6012
Acta méd. costarric vol.59 no.1 San José ene./mar. 2017
Articles
Epidemiological analysis of women with cervical squamous cell carcinoma 2007-2015
There is a marked difference between regions because of the sociocultural factors that surround each one. Lack of accessibility to health services, poor sex education, infrastructure and lack of knowledge greatly increase the risk of contracting the disease, since they involve risk factors that are closely associated with it. With a large gap between regions, even at the level of Latin America, there are marked differences between women, with worse diagnoses and prognoses in less favored regions.1,2 Therefore, it could be established that cervical cancer is a preventable disease, where sociocultural factors are determinants.
In Costa Rica, by 2014, cervical cancer ranked third in incidence, being more frequent in the provinces of San José, Alajuela and Heredia, and the fourth place in mortality by 2015, with Cartago and Alajuela being the provinces most affected, according to the National Registry of Tumors (NRT) and the National Institute of Statistics and Censuses (NISC).
Nationally, in 2006 it decreed mandatorily apply the system of screening with cervical cytology to women 20 years or older, sexually active biennially, and has shown favorable results in terms of reduction in incidence in cervix cancer in situ/cervical intraepithelial neoplasia grade 3 (CIN3). All women who initiate sex are at risk of being infected with the human papillomavirus, responsible for morphological changes that contribute to the development of cancer, and their prevalence has increased over the years.3 The screening program with cervical cytology, well applied, decreases cases of cervical carcinoma in situ and invasive, because it increases the early detection of preneoplastic lesions and hence, women are detected before they develop cancer. However, although the incidence of in situ cervical cancer / CIN3 declines, NRT documents that invasive carcinoma of the cervix shows a stable pattern over the years, suggesting that the screening program has not yet been able to be applied as desired and that there are women who escape early detection.4
In this article, the data was studied that was obtained from the archives of the Pathology Service of the Hospital Fernando Escalante Pradilla (PDEPH), which, being regional, provided coverage and support to the entire Brunca area, made up of the county of Perez Zeledón of San José and five counties of Puntarenas: Corredores, Coto Brus, Golfito, Osa and Buenos Aires. It is important to analyze the cervical epidermoid cancer behavior in this region, since it presents a type of population more susceptible to develop it, with greater difficulty for a screening process well established by problems of accessibility, loss of detection and less education. This work will allow you to document your pattern and which areas are most affected.
Study area
The Brunca region is located in the southeast of the country. It has an extension of 9528,4km2, for a 18.6% of the total in Costa Rica. According to the Central American Population Center of the UCR, it has a population of 296 308 inhabitants, corresponding to 6.2% of the population of the country, and is composed mostly by rural areas. The female population represents almost 50% of the total. Mideplan documents 24.6% of households living in poverty. Of those, 17.9% can not meet their basic needs, and 6.7% live in extreme poverty. According to age range, the NISC defines that for 2013, 57.2% is between 19-64 years old; 36.2%, less than 19 years, and 6.5% are over 65.
The United Nations Development Program points out that the Brunca Region is among the lowest educated and has a medium low human development index. All these data are characteristic of an area that has difficulty accessing health services, low socioeconomic level, low educational level and with limitation for an adequate prevention of pathologies such as cervical cancer.
The objective of this research work is to perform an epidemiological analysis of cervical cancer, using the data obtained from the PDEPH during the period 2007-2015. We want to establish the frequency of both carcinoma in situ/ CIN3 and invasive carcinoma of the cervix, and define the most frequent ages of presentation of cervical cancer. In addition, it is desired to determine the incidence of cervical cancer per county and the most frequent cytological interpretation, also by county.
Methodology
A retrospective study was conducted. Information from January 1, 2007 to December 31, 2015, was collected from the PDEPH, with a diagnosis of cervix epithelial carcinoma. The “Dr. Escalante Pradilla” hospital serves as a collection center for the other hospitals in the Brunca region, so the population studied comes from the six counties that compose it. In the Pathology Service, both the cytological interpretation and the diagnosis of biopsies are performed. For the study all women diagnosed with squamous cell cancer of the cervix during that period, for a total of 461 women were included, and excluded those diagnosed with adenocarcinomas. The variables to be studied were the type of cancer of the cervix (in situ/ CIN3 or invasive), the age at diagnosis and the year in which it occurred, the county of origin, if it had any cytology done two years prior to the diagnosis of cancer and which was the interpretation of this cytology. There were some women with more than one cytology within the two year period prior to the biopsy, so that only the most recent one was taken into account. The Bethesda system was used for cytological interpretation.
Calculations were made based on the female population distributed by county, published in the last census conducted by the NISC, and statistics of the NRT.
For 2011, the total female population was about 142 962; For 2012, of 171,909; In 2013, of 173,573; In 2014, with 172 105, and in 2015, with 176,852 women in the region (period of five years). Calculations of percentages, means, and rates, as well as graphs at work, were performed using the Microsoft Excel® 2016 worksheet for Windows.
Results
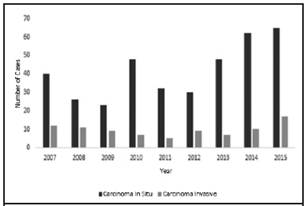
In the last nine years, a total of 461 cases of squamous cell carcinoma of the cervix were diagnosed in the PDEPH. Of these, 347 were carcinomas in situ (81%), compared to 87 cases of invasive carcinomas (19%), with a ratio of 4.29 to 1. (Figure 1). On average, 41.5 cases of carcinoma in situ and 9.6 cases of invasive carcinomas per year were diagnosed in the Brunca region. The average adjusted average per 100,000 women for cervical epidermoid carcinoma is 31 in the region (including 25 for carcinoma in situ and 6 for invasive carcinoma). As of 2012, there is an upward pattern in observing rates of epidermoid carcinoma of the cervix per year in the region (Figure 2).
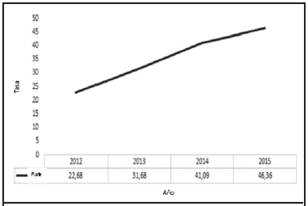
Figure 2 Incidence of squamous cell cervix carcinoma in the Brunca region from 2012. Adjusted rate per 100,000 women. A growing pattern has been observed over the last four years. Source: data collected from PDEPH
Carcinoma in situ comprises ages ranging from 18 to 87 years, with an average age of 38 years, with the age group having the highest number of cases is 26-30 years old, with 22% of carcinomas (n = 82). The mode is 30 years. Invasive carcinoma, on the other hand, comprises ages between 24 and 93 years, with an average of 50 years. The age group with the greatest number of cases is 46-50 years, corresponding to 16% of invasive carcinomas (n = 14). The mode is 46 years old. Globally, epidermoid cancer of the cervix affects the population of 26-30 years of age the most, with almost 20% (n = 88) (Figure 3).

Figure 3 Percent distribution of squamous cell cervix carcinoma, according to age group, Brunca region. Years 2007-2015. The age group of 26-30 years presents the majority of cases of carcinomas in situ and the 46-50 the most invasive carcinomas. Source: data collected from PDEPH
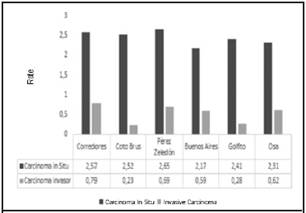
Figure 4 Incidence of squamous cell carcinoma of cervix Brunca region, by county. Rate adjusted by 10,000 women. Years 2007-2015. There are no large differences in county level. Source: data collected from PDEPH
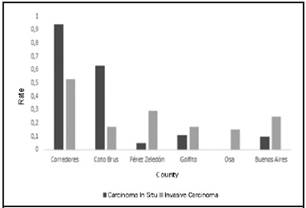
Figure 5 Incidence of women diagnosed with squamous cell carcinoma of the cervix without cytology, two years prior to diagnosis, according to county. Rate adjusted by 10,000 women. Years 2007-2015. Corredores and Coto Brus have the lowest cytological coverage. Source: data collected from PDEPH
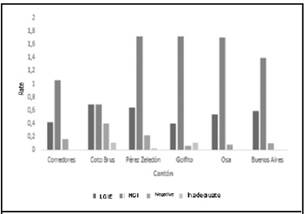
Figure 6 Adjusted rate for 10,000 women with cytological findings prior to the diagnosis of carcinomas in situ according to county. Years 2007-2015. The HGIEL is the one that predominates in the cytological interpretations preceding the carcinomas in situ. 1LGIEL: Low-grade intraepithelial lesion, 2HGIEL: High-grade intraepithelial lesion. Source: data collected from PDEPH
The incidence per county was estimated, as there are probably some areas with less coverage. By county, it was observed that the incidence for every ten thousand women resembles, being about 2 cases diagnosed by every ten thousand women, in all the counties (Figure 4). The highest incidence of carcinoma in situ occurred in the county of Pérez Zeledón, followed by Corredores and Coto Brus. Buenos Aires has the lowest rate. At the level of invasive carcinoma, Corredores was the one with the highest incidence, presenting a ratio of 1 invasive carcinoma per 3 in situ.
When analyzing the county distribution of cytological interpretations within the last two years prior to the diagnosis of epidermoid carcinoma of the cervix, differences in coverage with Papanicolaou are noted. The counties of Corredores and Coto Brus present the highest rate of women without cytology prior to diagnosis, and, according to percentage, women diagnosed with invasive carcinomas are the group with the lowest coverage, representing 47% (n = 41) (Figure 5). In each county, the highest interpretation rate corresponds to HGIEL with 59% (n = 219) of cytological interpretations, followed by low-grade intraepithelial lesions, with 26% (n = 86) (Figure 6). With regard to invasive carcinomas, the data obtained reflect differences according to the county. Corredores has a similar rate of cytological interpretations as HGIEL and inadequate collections. But in general, 60% (n = 23) of the cases are interpreted as predominantly HGIEL, followed by a negative 28% (n = 16) (Figures 5 and 7).
Discussion
Cervical cancer represents a global and social problem. The literature indicates that the statistics are higher in women from poor population groups with minimal schooling and living in developing countries, with Costa Rica being part of this group.5
Developed countries have well-established prevention, detection and control programs, so they have lower rates of cervical carcinoma. The high level of inequality at the global level, and in Costa Rica it can be verified even within the same country, propitiates the appearance of the disease.5
The Brunca region has all the characteristics of a socially disadvantaged area. At the beginning of the study, the socioeconomic characteristics were mentioned and why it represents a vulnerable area.
Projections indicate that the number of new cases will increase over the years, and Latin American countries will experience an increase of almost 75% of cases, only as a result of aging.6 The incidence rate for 2008 in the world was of 17.8 per 100,000 women, with almost 85% of deaths in developing countries.5
Nationally, compared to statistics of Sierra et al., from 1997 to 2008, cervical cancer has decreased,7 But from 2009-2014, data from the NRT show a relatively stable pattern in regards to incidence per 100.000, women from 2009-2014, being 31,73, 36,28, 29,44, 29,76, 32.11 and 29,33, respectively. The study shows that the incidente rate of cervical cancer in the Brunca region does not maintain a stable pattern at the national level during the study years, but reflects an upward pattern, mainly from 2012. This increase in The incidence in the total number of cervical carcinomas may be due to an improvement in coverage with cervical cytology, although the number of invasive cancers has not decreased, suggesting that although cytology coverage has improved, it is not yet The ideal. Over the years, the Brunca region has increased its contribution in diagnoses to national statistics, from representing 4.5% of cases diagnosed nationally in 2009, to 10.3% in 2014. It is shown that The frequency of diagnoses of both squamous cell carcinoma in situ / CIN3 and invasive carcinomas has increased and contributed to national statistics.
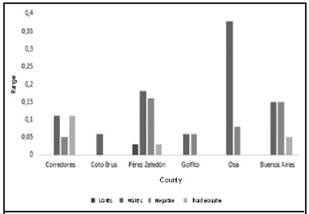
Figure 7 Rate adjusted by 10,000 women for cytological findings prior to the diagnosis of invasive carcinomas according to the county. Years 2007-2015. The most prevalent interpretation in the group of invasive carcinomas can not be defined with certainty. Source: data collected from PDEPH 1LGIEL: Low-grade intraepithelial lesion 2HGIEL: High-grade intraepithelial lesion
At the county level, the average rates during the nine years are similar. However, it is rescued that Corredores presents a higher rate of invasive carcinomas, but in turn also has the lowest level of cytological coverage, which provides an opportunity for its development. Presumably, an improvement in coverage may decrease the numbers of invasive carcinomas in these counties.
According to NRT statistics, since 2009-2014, the most affected age group at the national level is in the range of 35-39 years, followed by the 30-34 year old. The Brunca region presents a pattern of diagnosis in earlier ages, with the group being the most affected, overall, the 26-30 year old, with almost 20% (n = 88), followed by the group of 31-35 years , With 16%. Women diagnosed with invasive carcinoma are in a higher age range, 46-50 years, which can be attributed to the time that the disease needs to progress.8 These data can be found depending on the age of onset of sexual intercourse, the number of sexual partners, age at the beginning of screening to detect preneoplastic lesions, and attachment to the program.
Although there are several methods worldwide to perform screening, in the region under study conventional cytology is generally used.6 The Bethesda System is the most commonly used and is the most accepted for cytology reporting.9
Women in control with cervical cytology require multiple visits to the doctor over the years, correct collection of samples, colposcopies performed in due course, collection of biopsies, reporting results to patients and performing the indicated treatment. This requires infrastructure and proper handling of the samples. The Brunca region is a rural area, so it is necessary to travel from distant areas to the medical centers, to continue with their control and treatment, and that makes the process difficult.10
Studies in developing countries show that cervical cytology has a sensitivity of 31-78% and a specificity of 91-96%. These results are attributed to a combination of poor sample collection, incorrect preparation and errors in interpretation, since the results depend on the observer.11,12 However, although studies have shown low sensitivity and also false negatives, it has been shown that more important than the method used to screen, are the complete programs of prevention, monitoring and control.6
International statistics show that not all women go to screening. And in the United States inclusive, half of the new cases have never had a cytological test.13 Not all women, at the same time, continue with follow-up appointments.14
The Brunca region does not escape these figures, since 26.5% of the women studied did not have cytologies within the previous two years. The numbers are higher in the diagnoses of invasive carcinoma, giving opportunity for the disease to develop. Higher rates of lower coverage include the counties of Corredores and Coto Brus, which represent areas with difficult access to structured national programs. It is of the utmost importance to cover all the angles of the prevention program, since, as we have seen, not only involves cytology, but for efficient functioning, women must have adequate follow-up and control throughout time.
On the other hand, the literature has found a significant correlation between abnormal cytologies and histopathology.15 In regions of low socioeconomic status, cytology, colposcopy and histopathology should be used to better detect lesions.9 It has also been shown that conventional cytology is not appropriate for invasive neoplasms.14 The study correlates with this data, and most squamous cell carcinomas in situ/CIN3 have a previous interpretation of HGIEL, so ideally it has been mentioned that all women with abnormal cytological results should have a colposcopy.9 In 2015, a study was reported in the United States, which shows that, regardless of the method used, the most frequent diagnosis in women diagnosed with squamous cell carcinomas of the cervix was HGIEL.16 Previous cytologies in the diagnoses of invasive carcinomas don’t reveal any predominant interpretation, since, as mentioned, the cytology is not appropriate in invasive neoplasms.
It is concluded that the incidence of squamous cell carcinoma of cervix in the Brunca region has been increasing in recent years, and diagnoses of invasive carcinoma have not diminished. The most affected women represent a younger age group than the national population (26-30 years) and almost 26.4% of women did not have cytology within two years prior to the diagnosis of cancer. Women diagnosed with invasive carcinoma had a higher rate without previous cytology, which allowed the development of the disease. The Brunca region needs more help in sexual education and information about health to reduce the numbers presented, since it is a vulnerable area for the development of the pathology, due to the great socioeconomic component and, therefore, needs to increase strategies for fight it.
Work performed in: “Dr. Fernando Escalante Pradilla” Hospital
Abbreviations: PDEPH, Pathology Department of Escalante Pradilla Hospital; NRT, National Registry of Tumors; NISC, National Institute of Statistics and Censuses; HGIEL, high-grade intraepithelial lesion; CIN3, grade three cervical intraepithelial neoplasia
Affiliation: General practitioner.
Sources of support: Archive of the PDEPH
Conflicts of interest: There is no conflict of interest in this research work.nicolecaro9@gmail.com
Referencias
1. Capote Negrin L. Epidemiology of cervical cancer in Latin America. Ecancer medicalscience. 2015; 9:577. [ Links ]
2. Lina Villa L. Cervical Cancer in Latin America and the Caribbean: The Problem and the Way to Solutions. Cancer Epidemiol Biomarkers Prev. 2012; 21:1409-1413 [ Links ]
3. Rivas Suárez L. Virus del papiloma humano y cáncer de cuello de útero. Rev Méd Costa Rica. 2012; 129-132 [ Links ]
4. Ministerio de Salud. Normas y procedimientos de atención a la mujer para la prevención y manejo del cáncer de cuello de útero, para el I y II nivel de atención y normas de laboratorio de citología. 2006; 1-24 [ Links ]
5. Arzuaga Salazar M, Souza M, Azavedo Lima V. El cáncer de cuello de útero: un problema social mundial. Revista Cubana de Enfermería. 2012; 28(1):63-73 [ Links ]
6. Herrero R, Ferreccio C, Salmerón J et al. New Approaches to Cervical Cancer Screening in Latin America and the Caribbean. Vaccine. 2008; 26:49-58 [ Links ]
7. Sierra M, Soerjomataram I, Antoni S et al. Cancer patterns and trends in Central and South America. Cancer Epidemiology. 2016; 44:23-42 [ Links ]
8. DeVita V, Lawrence T, Rosenberg S. Cancer: Principles & Practice of Oncology. Editorial: Wolters Kluwer. Edición 9. 2011; 1311-1330 [ Links ]
9. Barut M, Kale A, Kuyumcuoglu et al. Analysis of Sensitivity, Specificity, and Positive and Negative Predictive Values of Smear and Colposcopy in Diagnosis of Premalignant and Malignant Cervical Lesions. Med Sci Monit. 2015; 21:3860-3867 [ Links ]
10. Murillo R, Almonte M, Pereira A et al. Cervical Cancer Screening Programs in Latin America and the Caribbean. Vaccine. 2008; 26:37-48 [ Links ]
11. Simion N, Caruntu I, Avadanei E, Balan R, Amalinei C. Conventional cytology versus liquid based cytology in cervical pathology: correspondences and inconsistencies in diagnosis, advantages and limits. Rom J Morphol Embryol. 2014; 55(4):1331-1337 [ Links ]
12. Alves C, Alves L, Lunet N. Epidemiology of Cervical Cancer. ArqiMed. 2010; 24(6):266-277 [ Links ]
13. Cheng W, Huang C, You S, Chen C, Hu C, Chen C. Clinical Significance of Cytologic Atypical Squamous Cells of Undetermined Significance. Obstet Gynecol. 2009; 113:888-894 [ Links ]
14. Sanabria Negrin J, Fernández Montequín Z, Cruz Hernández I, Oriolo Pérez L, Llanuch Lara M. El cáncer cervicouterino y las lesiones precursoras: revisión bibliográfica. Rev. Ciencias Médicas. 2011; 15(4):295-319 [ Links ]
15. Howell L, Tabnak F, Tudury AJ, Stoodt G. Role of Pap Test Terminology and Age in the Detection of Carcinoma Invasive and Carcinoma In Situ in Medically Underserved California Women. Diagn. Cytopathol. 2004; 30:227-234 [ Links ]
16. Miller R, Waters L, Mody D, Tams K. Squamous Cell Carcinoma of the Cervix A Cytology-Histology-Human Papillomavirus Correlation in Clinical Practice. Arch Pathol Lab Med. 2015; 139:776-781 [ Links ]
Received: September 21, 2016; Accepted: November 17, 2016
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
