










Serviços Personalizados
Journal
Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkActa Médica Costarricense
versão On-line ISSN 0001-6002versão impressa ISSN 0001-6012
Acta méd. costarric vol.58 no.1 San José Jan./Mar. 2016 Epub 01-Mar-2016
Original
Causal analysis for reentry of patients with hysterectomy
Gynecology Department, Hospital México, the Costa Rican Department of Social Security (CDSS). vivi.villagra08@gmail.com
Hysterectomy is a surgical procedure that is performed with great frequency; in the United States alone, there are about 600,000 such surgeries carried out every year.1 The rate of hysterectomy has varied between 6.1 and 8.6 per 1000 women in all age groups.2
It has been estimated that the prevalence of peri-operative complications associated with general gynecologic surgery ranges between 0.2% and 26.0%.3 Infection of the surgical site is the most common complication after any surgery, regardless of the reason for the surgery, of the type of procedure performed or of the surgical technique used.4
The risk of infection reported in the literature after a hysterectomy ranges approximately between 3 and 10%. On the other hand, the incidence of post hysterectomy surgical wound infection ranges between 3 and 8%. Post-hysterectomy infection is associated with morbidity ranging from 8 to 10%.5-6
It has been estimated that this procedure has a mortality rate of 8.6 per 100,000 abdominal hysterectomies and 2.7 for every 100,000 vaginal hysterectomies.7 Complete dehiscence of the fascia is associated with a mortality rate of 10% so that the latter situation is considered a surgical emergency.8
A majority of the relevant studies, mention an incidence of the surgical site after hysterectomy of between 4 and 12% in obese patients which is higher than the incidence in the non-obese population.9
In 1915, Brewer reported that rigorous aseptic procedures in the operating room could diminish the risk of infection of the surgical bed, measures which until the present time continue being used.10 It has been estimated that approximately 40 to 60% of infections of the surgical site can be prevented with an adequate administration of prophylactic antibiotics.11
Those patients who develop infection of the surgical site have a risk of re-admission that is five times greater, a risk of being admitted to an intensive care unit that is 60% greater as well as double the risk of dying, all of the above in comparison with patients who don´t develop this complication.12
At the present time, the rate of surgical site infection is being used as a parameter by means of which to evaluate the quality of attention being rendered by a hospital.13 These complications are the cause of hospital re-admission which in turn brings about an increase in the length of hospitalization, in the use of wide-spectrum antibiotics as well as in the need for undertaking new surgical procedures as well as an increase in the costs of care.5 The chances of re-admission for vaginal hysterectomy are approximately 2% and close to 1.6% for the abdominal approach ; both probabilities have gone up during the last two decades.14
An infection of the surgical site increases by 115.0% the hospitalization costs as compared with those seen in a non-infected patient.15 Gynecological surgery shows the lowest rate of surgical site infection (0.06%) in contrast to other surgical specialties (4.1%). More than 20.0% of readmissions are due to hemorrhage and 1.8% are due to infection.14 Hysterectomies done for benign conditions have been associated with a greater risk of complications and readmission.14
According to information provided by the Department of Statistics and Medical Records of the Hospital México (which is part of the Costa Rican Social Security System), a total of 4444 surgical procedures were performed in the Gynecology Service of this hospital between the years of 2009 and 2011. This represents an average of 1483 surgeries per year. Nevertheless, it is still unknown how many of these procedures are due to hysterectomies and how many of these patients were re-admitted. In addition, the cause for re-admission is unknown as are the risk factors associated with these events. The present study had as its purpose that of analyzing the most frequent causes for re-admission in patients with hysterectomy at the Gynecology Department of the Hospital México between January, 2009 and December, 2011.
Methods
A retrospective, descriptive study was carried out at the Gynecology Service of Hospital México and it inquired about the main causes of re-admission among patients older than 18 years of age in whom an abdominal, vaginal or laparoscopic hysterectomy had been performed by this Service. The main risk factors associated with the above procedures were also looked into.
The variables used were coded so as to allow for verification of the degree of statistical significance. Discrete variables were coded in such a fashion that would increase along with risk. The same criterion was applied to continuous variables so as to convert them into dichotomous and polytomous variables.
The main variables that were analyzed in this study were: age, body-mass index, presence of diabetes mellitus, hypertension, cancer, tobacco use, bacterial vaginosis, use of prophylactic antibiotics, operative time, length in days of hospital stay and need for repeat surgery or vacuum therapy.
Table 1: Distribution of socio-demographic variables among hysterectomized patients who were re-admitted to the Gynecology Service of the Hospital México between January, 2009 and December, 2011

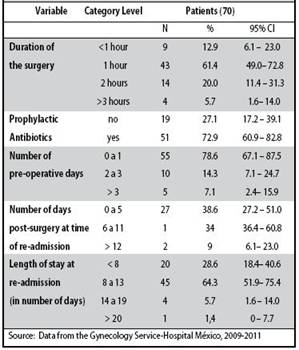
Table 2: Characteristics of the pre-operative, trans-operative and post-operative processes of patients re-admitted post-hysterectomy to the Gynecology Service of the Hospital México, between January, 2009 and December, 2011
The inclusion criterion to participate in the study was readmission to the Gynecology Service of Hospital Mexico, following a hysterectomy done between January, 2009 and December, 2011. Patients were excluded if the information was incomplete including, of course, if the chart had been lost.
An Excel database was designed and processed using the Epi Info statistical package (2002 version).
Approval was obtained, afte study and evaluation, by the Research and Bioethics Local Committee (CILOBI) belonging to the Women´s and Maternity Hospital called Adolfo Carit Eva.
Results
There were a total of 70 participants who fulfilled the inclusion criteria, who had complete.
Information in their charts and all of whom had undergone a hysterectomy in this Service.
The main variables that were analyzed are described in
Table 1. The largest age stratum or subgroup of hysterectomized patients who were re-admitted was that between 41 to 49 years of age.
The predominant body-mass index group was that between 26 and 30 and this group represented a full 41.4 percent of the total population of women. Regarding tobacco consumption, 91.4 percent didn’t have this habit. Of the remaining 8.6 percent of women who did smoke, greater than half of them were re-admitted because of infection of the surgical wound and in slightly over one tenth of them, the re-admission was due to a vaginal vault abscess. In addition, only 18.6% of the women studied, suffered from type two diabetes mellitus. In the latter population, an infectious cause was the main reason for re admission. On the other hand, 17.1 percent of the study participants, had some type of cancer and among them, about three quarters (12.8 percent) had as their cause for re-admission, an infection of the surgical site, thus making infection the main reason for hospitalization among this subgroup of women. Finally, 5.7 percent of the participants had bacterial vaginosis as their risk factor for the development of surgical site infection; all of the women who had pre-operative bacterial vaginosis received prophylactic antibiotics before the surgery and all of them developed an infection of the surgical wound that was associated with negative cultures.
With respect to the characteristics of both the preoperative and the trans-operative processes, Table 2 shows that the majority of the surgeries lasted longer than one hour but less than two hours and this was so in 61.4 percent of the cases.
A full 72.9 percent of the patients received prophylactic antibiotic treatment. The length of hospital stay during readmission ranged between 8 and 13 days of duration in 64.3 percent of the cases. 34.0% of the patients were re-admitted between 6 and 11 days after the surgery was performed and 38.6% of participants went back into the hospital between day 0 and day 5 of the post-operative period.
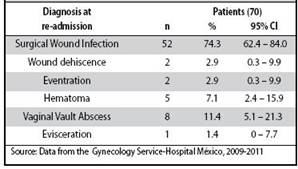
Table 3 shows that the main cause for re-admission of patients post-hysterectomy was surgical wound infection in 74.3% of cases followed by abscess of the vaginal vault in 11.8% of the women and, finally, evisceration and dehiscence of the surgical wound which, together, accounted for 2.9% of the re-admitted cases.
In only 60% of the participants was a culture of the surgical site taken at the time of re-admission. Besides, it was found that of all the patients in whom a culture at readmission was taken, only 48.6 percent of the results were reported in the chart.
The micro-organism most frequently isolated among the reported cultures was S. aureus which was found in 20.5 percent of the causal agents. Other bacteria (E. coli, Proteus, Klebsiella, Pseudomonas) constituted as a group, a full 79.5 percent of the causes of surgical site infection among the participants.
In 87.1% of the participants, a repeat surgical procedure was not done at re-admission. Only 12.9 percent (n=9) required such a re-intervention. In approximately 70 percent of the patients, vacuum therapy was performed so as to solve the infectious process.
Discussion
According to the literature, factors such as age, obesity, the presence of chronic illnesses such as diabetes or chronic obstructive pulmonary disease, predispose patients to postoperative infection.4
Age represents an independent variable as well as a nonmodifiable risk factor for the development of infection of the surgical site. Such an infection was present in women who were between 41 to 49 years of age, a fact which indicates that the majority of hysterectomies are performed in this age group, not only in our country but also elsewhere, as shown by the literature that was consulted.17
Morbid obesity is also associated with a higher rate of post-operative complications due to more complex as well as more prolonged procedures. Such a situation is consistent with the results obtained by Sherif et al, where morbid obesity was found to be an independent predictor of surgical site infection.
The majority of the patients in this study were not tobacco users, which coincides with the findings reported in the literature which directly implicate tobacco use with an increase in the risk of surgical site infection as well as inadequate post-operative wound tissue healing.19,20
In addition, post-operative hyperglycemia has been demonstrated to be an independent risk factor for the development of surgical site infection. There appears to be an already studied linear relationship between the degree of post-operative hyperglycemia and the risk of infection, a fact that coincides with the findings of the present study.21
A malignant tumor per se has limited effect on the healing of the surgical wound and this is confirmed by what other authors have found; nevertheless, malnutrition, reduced food intake and alterations in colonic function, all have a contribution to make in slowing the healing of the wound.17
We describe, in this study, a correlation between preoperative bacterial vaginosis and the risk of infection of the surgical wound. In this respect, it is worthwhile pointing out the importance of a recommendation issued by the American College of Obstetrics and Gynecology, that advises preoperative screening as well as treatment for bacterial vaginosis in all patients who are about to undergo a hysterectomy.22
An infection of the surgical wound represented the most frequent complication developed by the patients in the study and was the main cause for re-admission. These data confirm the observations by Faro and Faro, which indicate that the most relevant among the post-operative complications is infection of the surgical site.19
One tenth of the analyzed population showed another type of complication such as hematoma formation and evisceration. The literature mentions that post-hysterectomy evisceration occurs with a low frequency. It is estimated that its prevalence ranges between 0.032 and 1.2% and that it varies according to the surgical approach used.20, 23
According to Cruse and Ford at the National Research Council and Public Health Laboratory Service, there exists a direct relationship between surgical risk and the risk of post-operative infection since the latter doubles for each additional hour of duration of the procedure.24
At the Gynecology Service of Hospital México, three quarters of the study´s participants received pre-operative prophylactic antibiotics. According to the literature, the duration of such antibiotic therapy should be limited.26
Referencias
1. Cohen, S.L., Einarsson, J.I. Total and Supracervical Hysterectomy. Obstet Gynecol Clin N Am 2011; 38:651-661. [ Links ]
2. Berek, J. Ginecología de Novak. 14ª edición. Editorial Lippincott Williams & Wilkins. 2007; 829-871. [ Links ]
3. Lambrou, N.C., Buller, J.L., Thompson, J.R., Cundiff, G.W., Chou, B., Montz, F.J. Prevalence of perioperative complications among women undergoing reconstructive pelvic surgery. Am J Obstet Gynecol 2000; 183:1355-1360. [ Links ]
4. Fry, D.E., Fry, R.V. Surgical Site Infection: The Host Factor. AORN J. 2007; 86: 801-810. [ Links ]
5. Stany, M.P, Farley, J.H. Complications of Gynecologic Surgery. Surg Clin North Am. 2008; 88:343-359 [ Links ]
6. Kamat, A.A., Brancanzio, L., Gibson, M. Wound infection in Gynecologic Surgery. Infect Dis Obstet Gynecol. 2000; 8:230-234. [ Links ]
7. Hirsch, H.A., Kaser, O. Atlas de cirugía ginecológica con cirugía de mama, cirugía urológica y cirugía gastrointestinal. Editorial Marban. 2003; 123-152. [ Links ]
8. Millbourn, D., Cengiz, Y., Israelssson, L.A. Effect of stitch length on wound complications after closure of midline incisions: a randomized controlled trial. Arch Surg. 2009; 144:1056-1059. [ Links ]
9. Walsh, C., Scaife, C., Hopf, H. Prevention and Management of Surgical Site Infections in Morbidly Obese Women. Obstet Gynecol. 2009; 113:411-415. [ Links ]
10. Misteli, H., Weber, W.P, Reck, S., Rosenthal, R., Zwahlen, M., Fueglistaler, P., Bolli, M.K., Oertli, D., Widmer, A.F., Marti, W.R. Surgical Glove Perforation and Risk of Surgical Site Infection. Arch Surg. 2009; 144:553-558. [ Links ]
11. Hawn, M.T., Vick C.C., Richman, J., Holman, W., Deierhoi, R.J., Graham, L.A., Henderson, W.G., Itani, K.M. Surgical Site Infection Prevention. Time to move beyond the surgical care improvement program. Ann Surg. 2011; 254:494-501. [ Links ]
12. Salkind, A.R., Rao, K.C. Antibiotic prophylaxis to prevent surgical site infections. Am Fam Physician. 2011; 83: 585-590. [ Links ]
13. Fonseca, S.N., Kunzle, S.R., Junquiera, M.J., Nascimento, R.T., de Andrade, J.I., Levin, A.S. Implementing 1-dose antibiotic prophylaxis for prevention of surgical site infection. Arch Surg. 2006; 141:1109-1113. [ Links ]
14. Spilsbury, K., Hammond, I., Bulsara, M., Semmens, J.B. Mobility outcomes of 78577 hysterectomies for benign reason over 23 years. British Journal Obstetrics Gynecology 2008; 115:1473-1483. [ Links ]
15. Broex, E.C., van Asselt, A.D., Bruggeman, C.A., van Tiel, F.H. Surgical site infection: how high are the costs? J Hosp Infect. 2009; 72:193-201 [ Links ]
16. de Lissovoy, G., Fraeman, K., Hutchins, V., Murphy, D., Song, D., Vaughn, B.B. Surgical site infection: Incidence and impact on hospital utilization and treatment cost. Am J Infect Control. 2009; 37:387-97 [ Links ]
17. Pessaux, P., Msika, S., Atalla, D., Hay, J.M., Flamant, Y. Risk Factors for Postoperative Infectious Complications in noncolorectal abdominal surgery: a multivariate analysis based on a prospective multicenter study of 4718 patients. Arch Surg. 2003; 138:314-324. [ Links ]
18. El-Nashar, S., Diehl, C.L., Swanson, C.L., Thompson, R.L., Cliby, W.A., Famuyide, A.O., Stanhope, C.R. Extended antibiotic prophylaxis for prevention of surgical-site infections in morbidly obese women who undergo combined hysterectomy and medically indicated panniculectomy: a cohort study. Am J Obstet Gynecol. 2010; 202:306.e1-9 [ Links ]
19. Faro, C., Faro, S. Postoperative pelvic infections. Infect Dis Clin North Am. 2008; 22:653-663. [ Links ]
20. Ramírez, P.T., Klemer, D.P. Vaginal evisceration after hysterectomy: A literature review. Obstet Gynecol Surv. 2002; 57:462-467. [ Links ]
21. Ata, A., Lee, J., Bestle, S.L., Desemone, J., Stain, S.C. Postoperative hyperglycemia and surgical site infection in general surgery patients. Arch Surg. 2010; 145: 858-864. [ Links ]
22. Fry, D.E. A systems approach to the prevention of surgical infections. Surg Clin North Am. 2009; 89:521-537. [ Links ]
23. Croak, A.J., Gebhart, J.B., Klingele, C.J., Schroeder, G., Lee, R.A., Podratz, K.C. Characteristics of patients with vaginal rupture and evisceration. Obstet Gynecol 2004; 103: 572-576. [ Links ]
24. Hostetter, M.K. Handicaps to host defense. Effects of hyperglycemia on C3 and Candida albicans. Diabetes 1990; 39:271. [ Links ]
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
