










Servicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkActa Médica Costarricense
versión On-line ISSN 0001-6002versión impresa ISSN 0001-6012
Acta méd. costarric vol.58 no.1 San José ene./mar. 2016 Epub 01-Mar-2016
Original
28-day survival and mental and physical condition of patients discharged from a third level intensive care unit
Intensive Care Unit, Hospital “Dr. Rafael Ángel Calderón Guardia”, Caja Costarricense de Seguro Social, San José, Costa Rica. dasscom@gmail.com
Survival and quality of life following discharge from the Intensive Care Unit (ICU) are both frequent issues found in worldwide literature, but poorly explored in our country.
In general terms, ICU survival rates slowly improved throughout the years, deriving in a growing interest for medium and long-term effects in critical care survivors. The now called “post-ICU” syndrome1,2 involves a series of cognitive, functional and organic alterations, which present after an ICU stay, and cause important morbidity in these patients.
Also, intensive care is costly and consumes much of hospital resources, therefore it is fundamental to establish if this specialized and complex attention has an impact over these patients´ morbi-mortality after unit discharge.
Multiple epidemiological and experimental trials have focused their final goals at 28-day survival and health condition at the moment, making both well worth exploring points of interest.
The clinical condition for patients entering the ICU determines the existence of an important in-unit mortality, inherent to this population´s pathologies. However, once out of the unit, an adequate follow-up allows to predict the percentage of patients who will die sometime during the hospital stay, or during the first days out of the hospital. In the same way, it is important to know these patients´ quality of life and capability for social and work reintroduction. 3
This work presents the first survival and quality of life data for patients exiting the ICU during the rest of their hospital stay and 28 days after discharge; it is a major investigation that followed patients for a total of 6 months after discharge.
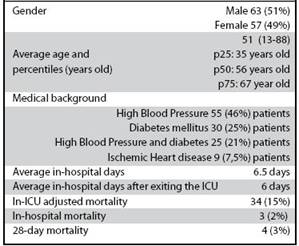
Table 1: General population characteristics for patients discharged from the Intensive Care Unit, 2014. n=120 patients
Objectives were to identify the study-group´s main socio-demographic characteristics and their health status when entering the ICU; to describe the patients´ ICU and hospital discharge condition, and to determine the quality of life for patients 28 days after exiting the hospital, parting from their independence and work reintroduction level, or their return to normal activities.
Methods
An observational, descriptive, prospective study, lasting one year, following all patients discharged from the ICU, with a 6 month enrollment period, from June to November 2014, and another 6 month follow-up period, until May 2015, with three cut points: at ICU discharge, at hospital discharge, and 28 days after. The gathered information included demographic and health condition data, collected at ICU admission and at the described cut points. Patients were interviewed, and in their absence, information was recalled from their caregivers. At the 28-day cut point, phone interviews were performed.
For ICU stay and mortality data, the Unit´s data base was used, and the rest of the information was gathered using a questionnaire written specifically for this study.
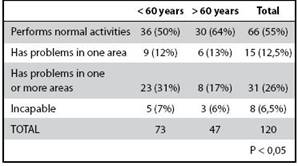
The ability to return to work and daily activities was explored establishing four categories: patients who resumed their previous conditions; patients who had only one reintroduction problem, either for self-care, physical mobility or for work; those with two or more problems in these areas, and those incapable of any reintroduction.
Statics analysis was performed with SPSS v.21 software (IBM Corp, USA).
This study was approved by the local bioethics committee, document number CLOBI-10-06-2014.
Results
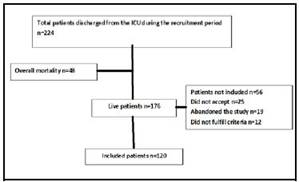
A total of 120 patients were recruited starting June 2014. Figure 1 summarizes the study enrollment flowchart.
Tables 1 and 2 show the main population characteristics, stay and mortality data, and the main diagnostic groups when admitted to the Unit. Regarding mortality, it is necessary to clarify that it corresponded to a 48 patient general mortality, but adjusted (excluding those patients who died during the first 24 hours after admission) mortality corresponded to 34 patients.
Table 2: Most frequent diagnoses from patients discharged from the Intensive Care Unit, 2014. n=120 patients
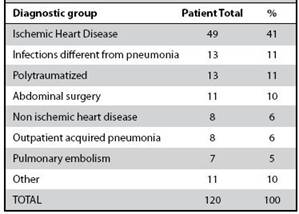
Table 2 shows the main diagnostic groups admitted to the Unit; 85 (71%) patients were entered the ICU from the medical area and 35 (29%) from the surgical area
There was no statistically significant difference between mortality, stay or diagnostic group for the patient´s gender.
Out of those patients who died and were still at the hospital, all of them died because of infectious causes (nosocomial pneumonia); out of discharged patients, one died because of sudden cardiac death, other died during hemodialysis, a third died because of hospital-acquired infectious endocarditis, and the last one did not receive a proven cause of death.
While the average ICU stay was 6.5 days, patients younger than 60 years had an 8-day average stay against 5.4 days in those over 60 years (p 0.001).
Cognitive condition at ICU discharge was adequate in 115 patients (96%); 3 were discharged in a state of confusion (2.5%), and 2 other patients in a vegetative state.
At ICU discharge, 66 patients (55%) were sent to different hospital services, 18 (15%) moved to another health center and 36 (30%) were discharged directly to their homes.
Table 3 presents the data on normal work reintegration, also separated by age, and it is remarkable that the best reintegration was from patients over 60 years (p <0.05).
There were no differences regarding gender either.
For those under 60 years, the lack of return to work was their main negative condition (17 patients), while social reintegration was for those over 60 (6 patients).
Discussion
It is always difficult to compare ICU units from different health centers and countries, as there are big differences between them, regarding the type of patients they receive (medical, surgical, oncological, coronary, mixed, etc), their admission and discharge criteria, complexity level, and demographic and pathological differences for the populations they attend.2,4,5 However it is important to compare the obtained information to worldwide published literature to look for similarities and differences.
Historically, of all patients admitted to the Hospital´s ICU, 65% are men and 35% women, because of the high and valetudinarian weight that ischemic heart disease has on men, which is also evident in the diagnostic groups where it is the main cause of income. However, in the patients studied, once discharged from the Unit, a very even gender distribution was found, so that no major statistical influence was found for gender on the length of stay, reintegration, or the final health condition. It also means that the most important mortality burden relies on men.
Worldwide literature provides little information on the cause of death of patients after ICU discharge,6 but sepsis, especially from a pulmonary focus, and respiratory failure of any origin, appear to be the most frequent causes of “post- ICU “death. In this study, at least for the rest of the hospital stay, these also appear to be the main causes of death. On the other hand, the mortality rate described of 5%, is lower than that reported at other centers, which could be encouraging regarding care received after ICU discharge.4,6,7
Regarding reintegration, it is clear that after 28 days still nearly half of patients are unable to achieve full or acceptable reintegration to normal activities, which could be linked to convalescence of the disease which forced them to be hospitalized. However, it is a conspicuous fact that patients over 60 years-old had a greater capacity for rehabilitation, and less problems in the different explored areas (self-care, physical and occupational mobility). Similar findings have been described by Jeitziner et al.8 in a recent study, which reported that elder patients who were in a Swiss medicalsurgical intensive care unit, however they had more postdischarge appointments, were less hospitalized or sent to specialized care homes. There seems to be a geriatric paradox, according to which, despite its age and comorbidities, geriatric patients survive better as they pass through intensive care units, although this is not a consistent finding.4,9
On the other hand, gender, length of stay, and even diagnosis, seem to have little to do with the reintegration ability, a finding that was also reported in an review by
Dowdy et al.9 in 2005, Cognitive status at the moment of discharge from the unit, seems to have a greater role as a reintegration capacity factor, 10 this should be confirmed by a study with a longer follow-up.
In conclusion, patients discharged from the ICU have a low mortality but with also low reintegration into their usual activities, perhaps in relation to their illness convalescence period. The health system appears to be very efficient to safeguard critically ill patients´ lives, although it may need to direct efforts towards patient monitoring in order to improve its recovery.
Referencias
1. Mehlhorn J, Freytag A, Schmidt K, Brunkhorst FM, Graf J, Troitzsch U, et al. Rehabilitation interventions for postintensive care syndrome: a systematic review. Crit Care Med. 45: 1263-71. doi: 10.1097/CCM.0000000000000148. [ Links ]
2. Jeitzine MM, Hantikainen V, Conca a, Hamers JPH. Long-term consequences of an intensive care unit stay in older critically ill patients: design of a longitudinal study. BMC Geriatr 2011; 11:52. doi: 10.1186/1471-2318-11-52. [ Links ]
3. Parker A, Sricharoenchai T, Needham DM. Early Rehabilitation in the Intensive Care Unit: Preventing physical and mental health impairments. Curr Phys Med Rehabil Rep. 2013; 1: 307-14. [ Links ]
4. Khouli H, Astua A, Dombrowski W, Ahmad, Homel, FP, Shapiro J, et al. Changes in health-related quality of life and factors predicting long-term outcomes in older adults admitted to intensive care units. Crit Care Med. 2011; 39: 731-7. doi: 10.1097/CCM.0b013e318208edf8. [ Links ]
5. Davidson JE, Harvey MA, Bemis-Dougherty A, Smith JM, Hopkins RO. Implementation of the Pain, Agitation, and Delirium Clinical Practice Guidelines and Promoting Patient Mobility to Prevent Post-Intensive Care Syndrome. Crit Care Med. 2013; 41:S136-45. [ Links ]
6. Braber A, van Zanten ARH. Unravelling post-ICU mortality: predictors and causes of death. Eur J Anaesthesiol. 2010; 27:486-90. doi: 10.1097/EJA.0b013e3283333aac. [ Links ]
7. Flaatten H. Mental and physical disorders after ICU discharge. Curr Opin Crit Care. 2010; 16:510-515. [ Links ]
8. Jeitziner MM, Zwakhalen SM, Hantikainen V, Hamers JP. Healthcare resource utilisation by critically ill older patients following an intensive care unit stay. J Clin Nurs .2015; 2:1347-56. doi: 10.1111/ jocn.12749 [ Links ]
9. Dowdy DW, Eid MP, Sedrakyan A, Mendez-Tellez PA, Pronovost PJ, Herridge MS, et al. Quality of life in adult survivors of critical illness: A systematic review of the literature. Intensive Care Med. 2005; 31:611-20. [ Links ]
10. Svenningsen H, Langhorn L, Ågård AS, Dreyer P. Post-ICU symptoms, consequences, and follow-up: an integrative review. Nurs Crit Care. 2015. doi: 10.1111/nicc.12165 [ Links ]
Received: March 30, 2015; Accepted: October 22, 2015
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
