










Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkActa Médica Costarricense
On-line version ISSN 0001-6002Print version ISSN 0001-6012
Acta méd. costarric vol.55 suppl.1 San José Jul. 2013
Conferencias Magistrales
Perspectivas sobre el diagnóstico de laboratorio de enfermedades rickettsiales en el siglo 21
Perspectives on the laboratory diagnosis of rickettsial diseases in the 21st century
Christopher D. Paddock
Resumen
Es necesario contar con métodos de laboratorio muy eficientes y específicos para poder distinguir las rickettiosis de otras enfermedades infecciosas y diferenciar con exactitud unas rickettsias de otras. Las categorías más importantes de métodos utilizados para diagnóstico de rickettsias son: Visualización directa por histología o tinciones inmunohistoquímicas, serología, cultivo y métodos moleculares, cada una de ellas posee sus fortalezas y debilidades. La presente revisión discute algunas de estas ventajas y desventajas inherentes a cada método y cómo estas técnicas pueden evolucionar colectivamente en el futuro. Históricamente, muchas enfermedades rickettsiales han sido pobremente estudiadas, generalmente porque estos patógenos se consideran difíciles de cultivar, difíciles de teñir y peligrosos de propagar en el laboratorio. Progresando hacia el siglo 21, un mayor uso de estos métodos de diagnóstico, especialmente en países tropicales y en vías de desarrollo podría beneficiar un reconocimiento global de las rickettsiosis y el impacto que estas tienen en un enorme segmento de la población mundial. Es cada vez más importante para los ricketsiólogos contemporáneos abstenerse de utilizar los métodos clásicos tales como cultivo, serología y hasta la visualización directa con la evolución de métodos moleculares más rápidos y sofisticados. Se pueden obtener resultados extraordinarios cuando se utilizan múltiples técnicas de manera concomitante.
Descriptores: Rickettsia, Ehrlichia, Orientia, Coxiella, diagnóstico
Abstract
Robust laboratory methods are necessary to distinguish rickettsioses from other infectious diseases and to accurately distinguish one rickettsiosis from another. The major categories of diagnostic techniques used for rickettsioses, i.e., direct visualization by histological or immunohistochemical stains, serology, culture, and molecular techniques, each have unique strengths and weaknesses. This review discusses some of the advantages and disadvantages inherent to each method and how these techniques might evolve collectively in the future. Many rickettsial diseases have been historically understudied, often because the pathogens were considered difficult to grow, difficult to stain, and dangerous to propagate. As we progress into the 21st century, the broader use of diagnostic assays, particularly in many tropical and developing countries, will better leverage the global recognition of rickettsioses, and the impact that these infections have on enormous segments of the world population. It will be increasingly important for contemporary rickettsiologists to refrain from replacing entirely classical methods such as culture, serology, or even direct visualization with more rapidly evolving and increasingly sophisticated molecular techniques. Extraordinary results can be achieved when multiple techniques are used in tandem.
Keywords: Rickettsia, Ehrlichia, Orientia, Coxiella, diagnosis
Laboratory diagnostics provide physicians with vital data that validate the accuracy of their clinical diagnoses and help define the true clinical spectrum of individual infections. These tools also occupy a fundamental role in the science of rickettsiology as drivers of pathogen discovery and by providing information necessary to uncover nuanced epidemiological and ecological features unique to each rickettsiosis. During the last decade, several publications have provided detailed descriptions of the various techniques used to diagnose the rickettsiosis,1-5 and the enormous downstream influence these assays have on epidemiological statistics for these diseases.6,7 The following discussion is not intended to comprehensively evaluate each method, but rather to emphasize some general strengths and weaknesses of the 4 major classes of these techniques, and how these might evolve collectively in the future.
Direct visualization
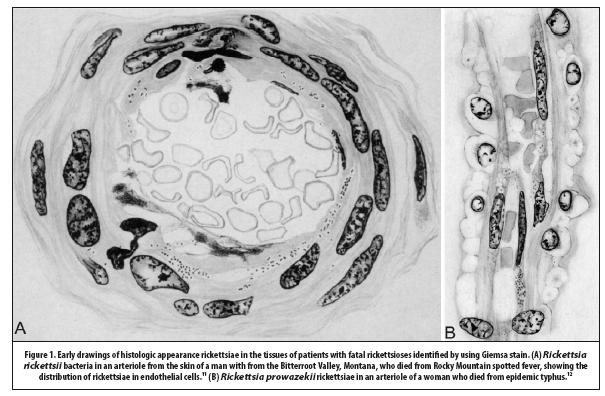
The small size, relatively sparse distribution and specific tinctorial properties of rickettsiae in tissues, blood, and other body fluids have historically posed challenges to clinicians and scientists attempting to visualize these pathogens in clinical samples. Howard Ricketts was the first to microscopically identify rickettsiae in animals and humans when he described “diplococcoid bodies, sometimes short bacillary forms” in Giemsa-stained smears of blood from patients with RMSF and guinea pigs and monkeys infected experimentally with Rickettsia rickettsii. 8,9 Ricketts was hesitant to state definitively that these structures were the etiologic agent of RMSF because he could not cultivate these bacteria by use of axenic media; nonetheless, his observations were soon corroborated by Simeon Burt Wolbach who used the same staining method to describe the characteristic appearance and distribution of rickettsiae in human tissues: …
“a short rod in pairs, joined end to end…found in apparently uninjured endothelium of normal vessels, in areas of proliferated endothelium of the intima of vessels, in hyaline necrosed intima in more advanced lesions, in apparently normal and necrosed smooth muscle fibers of vessels with lesions, and in endothelial cells in the perivascular zones of proliferation.”10
Traditional staining methods thus facilitated identification and description of the fundamental lesions of RMSF and louse-borne typhus (Figure 1), and provided a foundation for the pathophysiology of all vasculotropic rickettsiosis;11,12 nonetheless, the use of traditional histological stains as a diagnostic technique to detect rickettsiae in clinical samples is vanishingly rare in contemporary scientific and medical literature.13-15
In 1976, investigators first coupled hyperimmune animal serum with immunofluorescence techniques to detect spotted fever group (SFG) rickettsiae in tissues of ill patients;16 during the last 25 years, investigators have developed immunohistochemical (IHC) assays using monoclonal or polyclonal antibodies to identify various genera of rickettsial pathogens in formalin-fixed, paraffin-embedded biopsy or autopsy tissue specimens, including multiple SFG and typhus group (TG) Rickettsia species,17-23 E. chaffeensis,24-26 Anaplasma phagocytophilum24 and Orientia tsutsugamushi.27 Advantages of these methods include: (1) direct evidence of infection; (2) high sensitivity during the early stages of infection when other methods, particularly serology, are non-diagnostic; and, (3) excellent positive predictive value. The advantage provided by direct observation of the pathogen in the appropriate histopathological context is considerable and provides a second level of confirmation inherent only to this class of diagnostics.
Another useful and somewhat unique feature of IHC techniques is its application to specimens obtained years or even decades earlier. The cause of death of a Maryland patient from 1901 was confirmed ninety years later as RMSF by use of an IHC stain applied to archival paraffin-embedded tissues, predating retrospectively the first descriptions of this disease in the eastern United States by thirty years.28 Application of immunohistochemical techniques identified O. tsutsugamushi in archival tissues >50 years old.27 Finally, by identifying additional cellular targets of these pathogens, and by dissecting the specific inflammatory response of the vertebrate host, IHC techniques build on the foundation of rickettsial pathobiology established almost 100 years ago by conventional histological staining methods.19, 21, 26, 27 Disadvantages of IHC staining methods include: (1) the acquisition of the analyte, i.e., tissue, is typically more complex than collection of blood or serum; (2) the requirements of specimen processing and evaluation that often limit diagnostic capacity to specialized regional or national centers; and, (3) the use of immunologic reagents that are generally group-specific rather than species-specific.
Careful microscopical examination peripheral blood smears stained with eosin-azure type dyes will detect morulae in the cytoplasm of infected leukocytes in as many as 20%-30% patients infected with E. chaffeensis and approximately 20%-80% of those infected with Anaplasma phagocytophilum.29-31 The accuracy of these techniques is biased by the number of examined cells or blood smears, the level of immune compromise of the host, and the relative experience of the microscopist, who must distinguish morulae from other structures such as Döhle bodies, toxic granulations, or phagocytosed bacteria or fungi that may occur in the cytoplasm of white cells in other infectious conditions.29 This technique is relatively insensitive and inconsistent; however, its simplicity and ubiquity provided the initial discoveries of human monocytic ehrlichiosis and human anaplasmosis in the United States during the late 1980s and early 1990s.29, 31
Serology
Serological methods represent the most widely recognized, broadly available and frequently used tools for the diagnosis of rickettsial diseases; however, these techniques are also deeply ingrained in the minds of clinicians, often to the exclusion of any other category of confirmatory test. Despite the ease of use and accessibility of serological assays, these are distinguished from all other diagnostic methods by providing indirect evidence of infection or exposure, i.e., detecting host antibodies reactive with rickettsiae, rather than identifying directly antigens, nucleic acids, or live rickettsiae. The indirect immunofluorescence antibody (IFA) assay, generally considered the serological reference method for rickettsioses, was first applied for the diagnosis of murine and louse-borne typhus in 1959 and subsequent uses of IFA to diagnose other rickettsial diseases increased dramatically during the next several decades.32,33
The principal advantages of IFA, enzyme immunoassay (EIA), and other antibody detection methods include: (1) commercial availability; (2) relative simplicity; and, (3) opportunities for retrospective diagnosis weeks after the patient has recovered from the acute illness. Serologic methods can be used effectively to screen individuals and populations for rickettsial infections in regions where these diseases were previously unrecognized. By example, the recent identification of an unexpected and novel Orientia infection in a traveler to
Serological assays, particularly IFA methods, can be very effective at confirming rickettsial infections when 2 or more serum specimens are collected at appropriately timed intervals that generally range between 2 to 6 weeks, depending on the relative severity of the particular infection;35 however, when this protocol is not followed, the opportunities for misinterpreting data generated by serological assays are considerable, particularly when no other laboratory methods are included in the diagnostic evaluation of the patient. Paradoxically, serological methods are particularly insensitive during the acute stage of rickettsial infections, when most patients seek medical attention and when the majority of specimens are collected for subsequent evaluation by these techniques. As an example, initial serum samples collected from 11 of 22 patients with laboratory-confirmed rickettsialpox failed to demonstrate IgG antibody levels reactive with Rickettsia akari antigens at or above the conventionally recognized cutoff dilution when tested by using an IFA assay; confirmatory evidence of infection with R. akari in these 11 patients was obtained only because diligent clinicians collected additional specimens, including convalescent-phase serums and skin biopsy specimens for IHC, culture, and PCR.20Approximately 50% of patients with RMSF lack a diagnostically relevant IFA titer (i.e., > 64) during the first week of illness; however, at least half of all deaths attributed to R. rickettsii occur within 7-9 days after illness onset, explaining the large percentage of persons who die of RMSF without serological confirmation.18 In these circumstances, IFA methods have an exceptionally low negative predictive value and molecular methods (see below) can greatly enhance a diagnosis in cases of fatal disease, particularly if a serum sample collected during the acute illness is the only diagnostic specimen obtained by clinicians.36
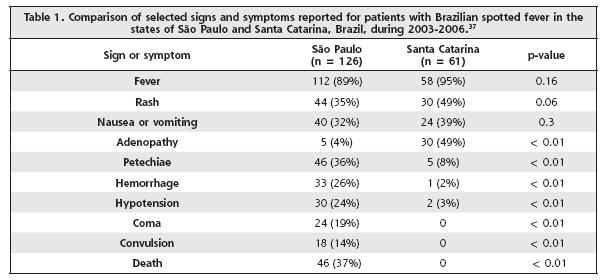
Patients infected with or exposed to Rickettsia, Ehrlichia, Anaplasma, Coxiella or Orientia species characteristically generate antibodies that are genus- or group-specific rather than species-specific. An important limitation of serological methods occurs when antibody titers are over-interpreted to ascribe a species-specific etiology based entirely on reactivity to a particular rickettsial antigen. In 2003, cases of Brazilian spotted fever (BSF) were reported for the first time in the state of Santa Catarina in southern
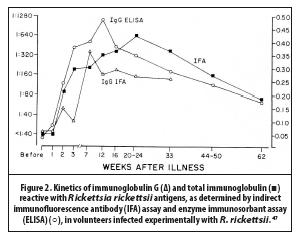
Serological diagnoses of rickettsioses are often confounded by the occurrence of preexisting levels of antibodies in the population at-risk that are reactive with a particular pathogen that may be different than the actual disease under investigation. In the United States, antibodies reactive with antigens of R. rickettsii occur at “diagnostic” levels in as many as 5% to 10% of the general population.42-46 There are several possible explanations for the serological noise created by diagnostically relevant antibody titers to pathogenic rickettsiae among otherwise healthy persons. These include serum reactivity with antigenically related but minimally or non-pathogenic species, and persistence of antibody levels among persons previously infected with or exposed to rickettsial antigens weeks, months, or perhaps years earlier (Figure 2).47
In some areas of the world the background seroprevalence to rickettsial agents is considerably higher. From separate studies in Colombia, approximately 40% of 392 randomly selected healthy adults in Cundinamarca Province demonstrated antibodies reactive with R. rickettsii at titers > 64 by using a well-validated IFA assay,48 while in Caldas Province, a staggering 490 (72%) of 682 sampled volunteers demonstrated IgG antibody titers > 64 to antigens of Rickettsia felis, Rickettsi typhi or both rickettsiae.49 In the Department of Loreto in the Amazon basin of Peru, a serosurvey of 1,195 persons during 2006 revealed antibodies reactive with SFG and TG Rickettsia species in 521 (43.6%) and 123 (10.3%) participants, respectively.50 Diagnostically relevant titers (i.e., > 64) to antigens of E. chaffeensis were identified among 15 (14%) of 105 healthy persons in a rural area of Jujuy Province, Argentina, despite the absence of any recently reported illnesses compatible with ehrlichiosis among the persons sampled.51
Serological methods, particularly IFA, are also subject to a lack of standardization among laboratories and inter-observer variability. A recent analysis of 109 published studies where IFA was used for the diagnosis of acute scrub typhus or to determine seroprevalance in a particular region found broad variation among studies with respect to the specific strains of O. tsutsugamushi used as antigen, the targeted antibody isotype, and the selection of cutoff titers that defined a positive result. In the majority of these studies no clear justification for the cutoff titer was provided. These authors concluded that no single antibody titer can reliably be considered diagnostic unless prior studies have been performed to determine the seroprevalence levels in the normal population of that locality.52 Important serological discrepancies occur even when identical specimens are evaluated by different laboratories. When a panel of serum specimens, collected from 52 persons 6 years after a point source outbreak of Q fever in Australia, were evaluated by IFA methods at 3 different international reference centers for serological evidence infection with Coxiella burnetii, the concordance status of IgG and IgM titers used to determine acute and chronic infections, past exposures, and serologically negative persons was only 35% among these highly respected laboratories.53
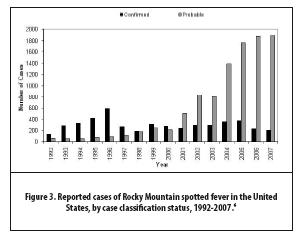
Nonetheless, serological methods are used with increasing frequency, often to the exclusion of other diagnostic tests. Results from these assays, most commonly represented as a single IFA titer or EIA absorbance value, are then used to generate epidemiological statistics; as a result, fewer cases are confirmed and a far greater percentage of cases are considered probable (Figure 3). The impact of diagnostic inaccuracy upon epidemiologic observations may be considerable. During 2000-2007, the reported case-fatality rate for RMSF in the United States was 0.5%, based on CRF denominator data comprising 7,796 cases, or approximately 1000 cases each year.6 One explanation for this estimate lies in the composition of the denominator, which is likely populated with patients with milder infections, caused by SFG Rickettsia species other than R. rickettsii.7
In some cases, western blotting and cross-adsorption techniques offer greater resolution with respect to the specific rickettsial pathogen; however, these assays are generally more expensive and technically difficult to perform, and are characteristically limited in availability to only a few reference centers around the world.3 In theory, cross-adsorption is the best serological method of identifying the specific rickettsial agent responsible for the infection and is based on the principle that homologous and heterologous antibodies will be removed entirely when the patient serum is incubated with the antigens of the specific pathogen responsible for the disease. When incubated with a heterologous antigen, only the group-specific antibodies responsible for the cross-reaction will be removed, whereas species-specific antibodies are retained. This technique has been used successfully to discriminate serologic responses to R. typhi from those to R. prowazekii.54 Nonetheless, the rationale for this technique can unravel when applied to SFG rickettsioses because: (1) the inherent pretest bias, i.e., an assumption that one of the antigens used in the assay is the pathogen responsible for the infection; and (2) the absence of appropriate positive and negative controls to validate the technique. In practice, most applications of the cross-adsorption technique assume only 2 possible pathogens, and the panel consists of 4 reactions; however, if correctly applied, adsorption panels must become considerably larger and more complex as additional SFG Rickettsia species are discovered and considered as potential pathogens. For example, if 3 sympatric SFG rickettsioses exist in a region, a panel should require 9 separate cross-adsorptions. If there are 4 possible agents, a correctly designed panel becomes prohibitively large with 16 separate reactions, which in practice is never observed. In this context, the utility of cross-adsorption is diminished in regions where there are multiple co-circulating and antigenically similar pathogens that cause similar clinical syndromes.
Culture
Culture represents the reference standard for microbiological diagnosis and is the least biased of all diagnostic techniques. Most pathogenic Rickettsia species will proliferate in many commonly used cell lines such as Vero E6 cells and human embryonic lung fibroblasts. The recent discovery of an axenic media for C. burnetii suggests that culture of other rickettsiae might also be achieved in carefully defined, cell-free mediums.55 Historically, rickettsiologists have been adept at culture techniques and these skills have resulted serendipitously in the isolation of several other important and novel non-rickettsial pathogens, including Legionella pneumophila, Tropheryma whipplei, and Heartland virus.56-58 Nonetheless, diagnostic laboratories are often reluctant to attempt isolation of rickettsial agents, founded largely on the perception of the dangers associated with this task. For much of the 20th century, cultivation of rickettsiae was inextricably linked with the unfortunate and surprisingly frequent occurrence of laboratory-acquired rickettsioses, often resulting in the death of the investigator. Rickettsioses accounted for approximately 15% of 3921 laboratory-associated infections and 14% of the infection-related deaths tabulated through 1974.59
Rickettsia typhi, R. prowazekii, O. tsutsugamushi, R. akari, R. africae, R. australis, and especially C. burnetii, have been associated with laboratory-acquired infections;59-67 however, it is the notoriety of R. rickettsii that instills the greatest fear among clinical microbiologists. During 1912-1942, 12 investigators in the
Nonetheless, it important to place these laboratory accidents in perspective: 20 (80%) of 25 fatal rickettsial infections occurred prior to 1945,59 before the availability of effective antibiotic therapy for these infections, and typically in circumstances lacking biological safety cabinets. Many of these deaths resulted from failure to use simple barrier precautions, such as disposable latex gloves, eye protection, or filtering facepieces. Finally, almost all laboratory-acquired rickettsioses have occurred in research facilities where: (1) large numbers of infected arthropods were housed for study or vaccine development;68 (2) massively infected cell cultures, embryonated chicken eggs, or animal tissues were manipulated by using unsafe techniques that generated infectious aerosols,60-62,64,65,70,71 or; (3) routine safety precautions and reporting of laboratory accidents were not followed.63,66,69 These facilities and circumstances are far different than those reasonably expected in a routine diagnostic laboratory. Finally, it is should also be noted that through 1974, there were 439 cases and 40 deaths attributable to laboratory-associated typhoid, leptospirosis, and psittacosis,59 to underscore the fact that cultivation of any pathogenic agent posed far greater risks to microbiologists before the implementation of the safeguards and guidelines that are now used in diagnostic laboratories around the world.
Biosafety level-3 practices and facilities are currently recommended for diagnostic activities involving the manipulation of known or potentially infectious materials and for inoculation and incubation of cell cultures with any recognized pathogenic Rickettsia, Orientia, or Coxiella species.72 For exquisitely infectious agents such as C. burnetii, and highly virulent rickettsiae such as R. prowazekii and R. rickettsii, this level of containment seems justified. However, different species of Rickettsia vary greatly in pathogenicity, and a rational application of species-specific rather than genus-wide recommendations for cultivating rickettsial agents deserves some consideration in the future, particularly if more clinical laboratories are ever expected to pursue culture isolation as a contemporary diagnostic technique. Microbiologists are confronted continuously with pathogens that pose some level of occupational risk. As an example, Neisseria meningitidis is classified as a biosafety level 2 pathogen;72 nonetheless, 18 cases of laboratory-acquired meningococcal disease, including 8 deaths, were identified in laboratories around the world during 1985-2002, predominantly among laboratorians who worked with isolates on an open benchtop.73 An argument might be made that the hazards associated with some rickettsial pathogens are no greater, and quite possibly less, than those associated with N. meningitidis, particularly if all work is performed using a biological safety cabinet. One additional level of complexity was alleviated in December 2012, when R. rickettsii was removed from the list of select agents, so that possession, storage, or transfer of cultures infected with this pathogen no longer require registration with and oversight by the Centers for Disease Control and Prevention.74
Molecular methods
“In the years ahead, as we compare the nucleotide sequences of various rickettsiae, it should be possible to develop group-specific, species-specific, and perhaps even strain-specific probes that can be used both for diagnosing diseases and for conducting precise epidemiologic investigations.”75
It is perhaps difficult to imagine a time when molecular tools were not routinely available to rickettsiologists; yet as recently as 1991, as suggested by Joseph McDade, these resources could only be imagined. In 2013, the genetic codes unique to each species, subspecies, and strain of rickettsiae provide the foundation for confirmatory diagnosis and molecular epidemiology of the rickettsioses, and represent the cornerstone of pathogen discovery in this discipline. Largely because of the revolution in molecular biology and its direct application to rickettsiology, the number of distinct Rickettsia, Orientia, Ehrlichia, and Anaplasma spp. recognized as pathogens of humans has more than doubled since 1985.
Molecular techniques have been instrumental in epidemiological assessments of the origins of outbreaks and distributions of subtypes or strains. A devastating outbreak of RMSF that occurred during 2008-
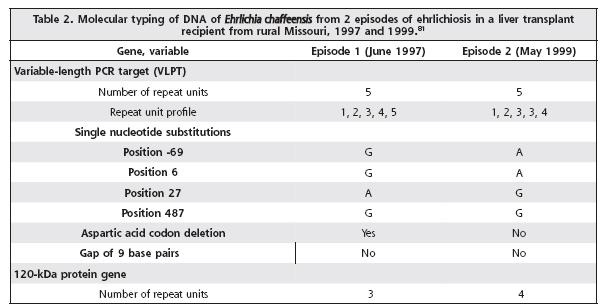
The granularity of molecular methods allows careful assessment of clinical features of specific rickettsioses that were previously obscured by less specific assays. In a recent study, investigators used molecular methods to accurately diagnose 140 consecutive Portuguese patients with Mediterranean spotted fever. The case-fatality rate in this series, determined by using specific diagnostic assays, was 21%, more than 8 times greater than the previously recognized lethality of this disease. In addition, they identified a particular strain of R. conorii that was more frequently associated with severe disease in this patient population.80Molecular methods can be used to examine the natural history and disease dynamics of rickettsioses. The first description of confirmed reinfection of a human host with E. chaffeensis was identified by using molecular techniques.81 A 56-year-old liver transplant reciepient from a rural area of Missouri developed laboratory confirmed ehrlichiosis in 1997 and 1999. Whole blood specimens collected during each episode were evaluated separately by using PCR and sequence analysis to determine the nucleotide pattern of the variable-length PCR target (VLPT) and 120-kDa genes of E. chaffeensis present in each sample. Because the VLPT and 120-kDa antigen genes demonstrate a variety of strain-specific patterns, it could be determined conclusively that the 2 episodes resulted from infections with separate and distinct strains of E. chaffeensis, rather than recrudescence of a persistent infection (Table 2).81
The sensitivity and specificity of molecular methods have been enhanced considerably by continuously evolving technologies, including real-time and loop-mediated isothermal PCR techniques.82-86 It has been proposed that these types of diagnostic tests can be implemented easily in laboratories with basic molecular capacity and developed as acute point-of-care assays.84,85 Highly specific molecular assays have great utility in regions where particular rickettsial pathogens are known to be endemic; however, broad-range molecular methods can be extremely useful in some circumstances, particularly when multiple, genetically distinct agents occur sympatrically, or in regions where the existence of a novel rickettsiosis is unrecognized. In
The acquisition and evaluation of clinical samples previously not considered, or believed suboptimal for a particular molecular method, are recognized increasingly as important sources of diagnostic information. Concentration of rickettsiae by centrifugation of serums of infected animals was first described by Ricketts in 1909;9 today, cellular sediments obtained from serum represent just one of many non-conventional specimens used increasingly as successful sources of template for molecular assays. This technique has been used effectively to provide diagnostic material for PCR-confirmation of various rickettsioses, including RMSF,36,77,79 Israeli spotted fever,89 Thai tick typhus,90,91 Rickettsia felis rickettsiosis,92,93 and scrub typhus.83 Improvements in nucleic acid extraction technology permit better recovery of rickettsial DNA from formalin-fixed, paraffin-embedded skin biopsy or autopsy tissues to allow species-specific PCR assays. Included among infections confirmed recently by using this technique are those caused by R. rickettsii,94,95 R. parkeri96 and Rickettsia 364D.97
The use of swabs to collect rickettsial nucleic acids from eschars and vesicular rash lesions for PCR analysis was first described in 2009.98 Subsequent reports described successful application of this simple and minimally invasive method to confirm cases of Queensland tick typhus,67 African tick bite fever,67,99 Mediterranean spotted fever,100 R. parkeri rickettsiosis,101 and Rickettsia 364D rickettsiosis.102 Eschar swabs represent highly versatile specimens that can provide confirmatory results retrospectively from healing lesions, in some cases as long as 2 weeks after initiation of antibiotic therapy.98,101 Because the technique is more rapid, easier to perform, and generally less painful than biopsy techniques, there is greater patient and physician acceptance, particularly in areas with limited medical resources;67,100 Scab material from the eschar surface may also provide a source of rickettsial DNA suitable for molecular confirmation.103 Despite these important advantages, eschar swabs should not be considered categorically as a replacement for cutaneous biopsy methods, for unlike swab material, tissue specimens provide histological context that may assist in an alternate diagnosis if the skin lesion is caused by something other than a Rickettsia species.104 Skin biopsy techniques also allow for cultivation of rickettsiae from the clinical specimen and are more likely than swabs to provide confirmatory results by molecular evaluation.22,67,104
Prospectus
Improving access to and awareness of species-specific diagnostic methods remain important challenges for 21st century rickettsiologists. Broader use of these techniques around the world might change considerably existing notions about the ecology, epidemiology, and clinical presentations of many rickettsioses. During the last 30 years, adherence to this principle has leveraged the discovery of >20 newly recognized rickettsioses and has clarified several long-standing epidemiologic questions about the clinical heterogeneity and unusual geographical distributions of many historically recognized rickettsial diseases.
In regions of the world where malaria, typhoid, leptospirosis, or dengue are endemic, there is accumulating evidence that rickettsial diseases also circulate with considerable frequency, embedded as misdiagnosed cases among statistics for these other, more classically recognized tropical diseases. By example, 10% of Cameroonian patients with undifferentiated febrile illnesses for whom malaria and typhoid were excluded had molecular evidence of infection with E. chaffeensis.105 During a serological study in the states of Jalisco and Yucatan in Mexico, an astounding 20 (40%) of 50 of patients with a clinical diagnosis of dengue had robust antibody titers reactive with SFG Rickettsia species, yet no demonstrable antibodies reactive with dengue virus.106 In a similar manner, serological evidence of recent infections with SFG Rickettsia species was identified in 22% of 96 serum samples collected during 2000-2001 as part of regional surveillance for dengue in Cundinamarca, Colombia. 107 Two confirmed and 7 probable cases of R. parkeri rickettsiosis in Argentina were identified by careful laboratory evaluation of patients presenting to one hospital with fever, myalgias and rash, several of whom were diagnosed initially with leptospirosis or dengue.108
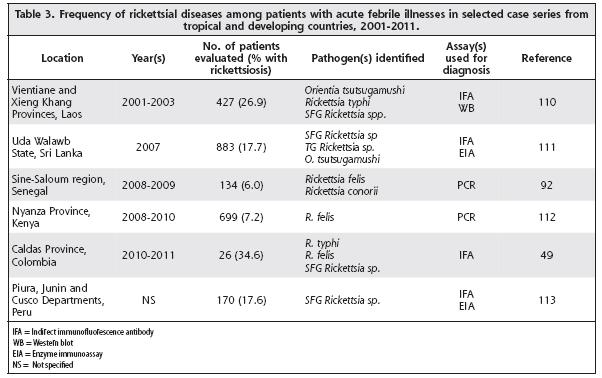
The scope and magnitude of rickettsial infections in many densely populated and geographically diverse areas of the world including India, Africa, Southeast Asia, and Central and South America remain poorly understood, yet during the last decade, diagnostic tools have uncovered a plethora of agents and diseases that impact the health of populations in these regions.109 The rigorous and routine use of rickettsial diagnostics in several prospective studies of febrile patients in these understudied regions has unveiled a surprisingly high prevalence of rickettsioses in these areas and signals an interesting and important period of discovery (Table 3). The frequency of undetected rickettsioses may be even greater when diseases associated with fever and cutaneous eruptions are investigated by these methods. During a prospective study at 2 hospitals in eastern Algeria, 108 adults who presented with fever and rash during 2000-2006 were evaluated for laboratory evidence of a rickettsiosis; acute infection with a SFG or TG Rickettsia species was confirmed in 14 (13%) of 108 enrolled patients during this interval.114 Confirmatory evidence of SFG rickettsioses was obtained from PCR analysis of skin biopsy specimens obtained from 24 (58.6%) of 58 consecutive patients with fever and rash who presented for care at a hospital in Tamil Nadu State, India, during 2006-2008.115
Many rickettsial diseases have been historically understudied, often because the agents were considered difficult to grow, difficult to stain, and dangerous to propagate. As we progress into the 21st century, the diagnostic techniques outlined above will leverage the global recognition of rickettsial diseases and the impact that these have infections on enormous segments of the world population. Each method has unique strengths, and it is important for rickettsiologists to refrain from replacing entirely classical methods with rapidly evolving and increasingly sophisticated molecular techniques. The pitfall of routinely relying on a single diagnostic method was recognized by Pijper and Crockett in 1938,116 when they stated,
“Different authors stress different methods of approach, and few use all of them…In Rickettsioses (sic) research, few methods are conclusive when used by themselves. There are so many approaches, and it is unfortunate that different workers value them differently…Identical methods are not always applicable to the various diseases. Only then can a Rickettsiosis (sic) be said to have been completely studied when all possible approaches have been explored.”
Pursuits in rickettsiology are most successful when traditional and contemporary methods are used in a complementary approach. Despite some specific and defined limitations inherent to each of the classes of rickettsial diagnostic methods, extraordinary results are achieved when multiple techniques are used in tandem. As an example, when high titers of antibodies reactive with E. chaffeensis were detected among a cohort of ill patients in Wisconsin and Minnesota, who presented with classical signs and symptoms of ehrlichiosis but who resided hundreds of miles beyond the established range of the recognized tick vector of E. chaffeensis, the application of cell culture and molecular techniques subsequently revealed a newly recognized ehrlichial pathogen in the United States.117 Laboratories that develop expertise in and routinely apply multiple combinations of these methods provide the highest level of diagnostic accuracy and are positioned characteristically at the leading edge of discovery.
Disclaimer: The findings and conclusions are those of the author and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
References
1. Brouqui P, Bacellar F, Baranton G, Birtles RJ, Bjoërsdorff A, Blanco JR, et al. Guidelines for the diagnosis of tick-borne bacterial diseases in Europe. Clin Microbiol Infect 2004; 10:1108-1132. [ Links ]
2. Chapman AS, Bakken JS, Bloch KC, Buckingham SC, Dasch GA, Dumler JS, et al. Diagnosis and management of tickborne rickettsial diseases: Rocky Mountain spotted fever, ehrlichioses, and anaplasmosis—United States: a practical guide for physicians and other health-care and public health professionals. MMWR 2006; 55:1-29. [ Links ]
3. Fenollar F,
4. Richards AL. Worldwide detection and identification of new and old rickettsiae and rickettsial diseases. FEMS Immunol Med Microbiol 2012; 64:107-110. [ Links ]
5. Eremeeva ME. Molecular epidemiology of rickettsial diseases in
6. Openshaw JJ, Swerdlow DL, Krebs JW, Holman RC, Mandel E, Harvey A, et al. Rocky Mountain spotted fever in the United States, 2000-2007: interpreting contemporary increases in incidence. Am J Trop Med Hyg 2010; 83:174-182. [ Links ]
7. Paddock CD,
8. Ricketts HT. A micro-organism which apparently has a specific relationship to
9. Ricketts HT,
10. Wolbach SB. The etiology of
11. Wolbach SB. Studies on
12. Wolbach SB, Todd JL, Palfrey FW. The etiology and pathology of typhus.
13. Castleman B, Scully RE, McNeely BU. Case records of the
14. Stasko T, De Villez RL. Murine typhus: a case report and review. J Am Acad Dermatol 1982; 7:377-381. [ Links ]
15.
16. Woodward TE, Pedersen CE, Oster CN, Bagley LR, Romberger J, Snyder MJ. Prompt confirmation of Rocky Mountain spotted fever: identification of rickettsiae in skin tissues. J Infect Dis 1976; 134:297-301. [ Links ]
17. Dumler JS, Gage WR, Pettis GL, Azad AF, Kuhadja FP. Rapid immunoperoxidase demonstration of Rickettsia rickettsii in fixed cutaneous specimens from patients with Rocky Mountain spotted fever. Am J Clin Pathol 1990; 93:410-414. [ Links ]
18. Paddock CD, Greer PW, Ferebee TL, Singleton J, McKechnie DB, Treadwell TA, et al. Hidden mortality attributable to Rocky Mountain spotted fever: immunohistochemical detection of fatal, serologically unconfirmed disease. J Infect Dis 1999; 179: 1469-76. [ Links ]
19. Walker DH,
20. Paddock CD, Zaki SR, Koss T, Singleton Jr. J, Sumner JW, Comer JA, et al. Rickettsialpox in
21. Lepidi H,
22. Paddock CD, Finley RW, Wright CS, Robinson HN, Schrodt BJ, Lane CC, et al. Rickettsia parkeri rickettsiosis and its clinical distinction from Rocky Mountain spotted fever. Clin Infect Dis 2008; 47:1188-1196. [ Links ]
23. Walker DH, Feng HM, Ladner S. Billings AN, Zaki SR, Wear DJ, et al. Immunohistochemical diagnosis of typhus rickettsioses using an anti-lipopolysaccharide monoclonal antibody. Mod Pathol 1997; 10:1038-1042. [ Links ]
24.
25. Dawson JE, Paddock CD, Warner CK, Greer PW, Bartlett JH, Ewing SA, et al. Tissue diagnosis of Ehrlichia chaffeensis in patients with fatal ehrlichiosis by use of immunohistochemistry, in situ hybridization, and polymerase chain reaction. Am J Trop Med Hyg 2001; 65:603-609. [ Links ]
26. Smith Sehdev AE, Dumler JS. Hepatic pathology in human monocytic ehrlichiosis. Am J Clin Pathol 2003; 119:859-865. [ Links ]
27.
28. Dumler JS.
29. Paddock CD, Childs JE. Ehrlichia chaffeensis: a prototypical emerging pathogen. Clin Microbiol Rev 2003; 16:37-64. [ Links ]
30. Childs JE, Sumner JW, Nicholson WL, Massung RF, Standaert SM, Paddock CD. Outcome of diagnostic tests using samples with culture-proven human monocytic ehrlichiosis: implications for surveillance. J Clin Microbiol 1999; 37:2997-3000. [ Links ]
31. Bakken JS, Dumler JS. Human granulocytic anaplasmosis. Infect Dis Clin N Am 2008; 22:433-488. [ Links ]
32. Goldwasser RA, Shepard CC. Fluorescent antibody methods in the differentiation of murine typhus and epidemic typhus sera: specificity changes resulting from previous immunization. J Immunol 1959; 82:373-380. [ Links ]
33. Philip RN, Cassper EA, Ormsbee RA, Peacock MG, Burgdorfer W. Microimmunofluorescence test for the serological study of Rocky Mountain spotted fever and typhus. J Clin Microbiol 1976; 3:51-61. [ Links ]
34. Izzard L, Fuller A, Blacksell SD, Paris DH, Richards AL, Aukkanit N, et al. Isolation of a novel Orientia species (O. chuto sp. nov.) from a patient infected in Dubai. J Clin Microbiol 2010; 48:4404-4409. [ Links ]
35. Fournier PE, Jensenius M, Laferl H, Vene S, Raoult D. Kinetics of antibody responses in Rickettsia africae and Rickettsia conorii infections. Clin Diag Lab Immunol 2002; 9:324-328. [ Links ]
36. dos Santos FCP, do Nascimento EMM, Katz G, Angerami RN, Colombo S, de Souza ER, et al. Brazilian spotted fever: real-time diagnosis PCR for fatal cases. Ticks Tick Borne Dis 2012; 3:312-314. [ Links ]
37. Angerami RN, da Silva AMR, Nascimento EMM, Colombo S, Wada MY, dos Santos FCP, et al. Brazilain spotted fever: two faces of the same disease? A comparative study of clinical aspects between an old and a new endemic area in
38. Gehrke FS, Nascimento EMM, de Souza ER, Colombo S, da Silva LJ, Schumaker TTS. Detection of Rickettsia rickettsii and Rickettsia sp. in blood clots in 24 patients from different municipalities of the state of
39. Medeiros AP, de Souza AP, de Moura AB, Lavina MS, Bellato V, Sartor AA, et al. Spotted fever group Rickettsia infecting ticks (Acari: Ixodidae) in the state of Santa Catarina, Brazil. Mem Inst Oswaldo Cruz 2011; 106:926-930. [ Links ]
40. Spolidorio MG, Labruna MB, Mantovani E, Brandão PE, Richtzenhain LJ, Yoshinari NH. Novel spotted fever group rickettsiosis, Brazil. Emering Infect Dis 2010; 16:521-523. [ Links ]
41. Silva N, Eremeeva ME, Rozental T, Ribeiro GS, Paddock CP, Ramos EAG, et al. Eschar-associated spotted fever rickettsiosis, Bahia, Brazil. Emerging Infect Dis 2011; 17:275-278. [ Links ]
42. Wilfert CM, MacCormack JN, Kleeman K, Philip RN, Austin E, Dickinson V, et al. The prevalence of antibodies to Rickettsia rickettsii in an endemic area for
43. Taylor JP, Tanner WB, Rawlings JA, Buck J, Elliott LB, Dewlett HJ, et al. Serological evidence of subclinical Rocky Mountain spotted fever infections in Texas. J Infect Dis 1985; 151:367-369. [ Links ]
44. Hilton E, DeVoti J, Benach JL, Halluska ML, White DJ, Paxton H, et al. Seroprevalence and seroconversion for tick-borne diseases in a high-risk population in the Northeast United States. Am J Med 1999; 106:404-409. [ Links ]
45. Marshall GS, Stout GG, Jacobs RF, Schutze GE, Paxton H, Buckingham SC, et al. Antibodies reactive to Rickettsia rickettsii among children living in the southeast and south central regions of the United States. Arch Pediatr Adolesc Med 2003; 157:443-448. [ Links ]
46. Graf PFC, Chretien JP, Ung L, Gaydos JC, Richards AL. Prevalence of seropositivity to spotted fever group rickettsiae and Anaplasma phagocytophilum in a large, demographically diverse
47. Clements ML, Dumler JS, Fiset P, Wisseman Jr. CL, Snyder MJ, Levine MM. Serodiagnosis of Rocky Mountain spotted fever: comparison of IgM and IgG enzyme-linked immunosorbent assays and indirect fluorescent antibody test. J Infect Dis 1983; 148:876-880. [ Links ]
48. Hildago M, Sánchez R, Orejuela L, Hernández J, Walker DH, Valbuena G. Prevalence of antibodies against spotted fever group rickettsiae in a rural area of
49. Hildago M, Montoya V, Martínez A, Mercado M, De la Ossa A, Vélez C, et al. Flea-borne rickettsioses in the North of Caldas Province, Colombia. Vector-Borne Zoonotic Dis 2013; 13:289-294. [ Links ]
50. Forshey BM, Stewart A, Morrison AC, Gálvez H, Rocha C, Astete H, et al. Epidemiology of spotted fever group and typhus group rickettsial infection in the Amazon
51. Ripoll CM, Remondegui CE, Ordonez G, Arazamendi R, Fusaro H, Hyman MJ, et al. Evidence of spotted fever and ehrlichial infections in a subtropical
52. Blacksell SD, Bryant NJ,
53. Healy B, van Woerden H, Raoult D, Graves S, Pitman J, Lloyd G, et al. Chronic Q fever: different serological results in three countries—results of a follow-up study 6 years after a point source outbreak. Clin Infect Dis 2011; 52:1013-1019. [ Links ]
54. La Scola B, Rydkina L, Ndihokubwayo JB, Vene S, Raoult D. Serological differentiation of murine and epidemic typhus using cross-adsorption and western blotting. Clin Diag Lab Immunol 2000; 7:612-616. [ Links ]
55. Omsland A,
56. McDade JE, Shepard CC, Fraser DW, Tsai TR, Redus MA, Dowdle WR, et al. Legionnaire’s disease. Isolation of the bacterium and demonstration of its role in other respiratory disease. N Engl J Med 1977; 297:1197-1203. [ Links ]
57. Raoult D, Birg ML, La Scola B, Fournier PE, Enea M, Lepidi H, et al. Cultivation of the bacillus of Whipple’s disease. N Engl J Med 2000; 342:620-625. [ Links ]
58. McMullan LK, Folk SM, Kelly AJ, MacNeil A, Goldsmith CS, Metcalfe MG, et al. A new phlebovirus associated with severe febrile illness in
59. Pike RM. Laboratory-associated infections: summary and analysis of 3921 cases. Health Lab Sci 1976; 13:105-114. [ Links ]
60. Sulkin SE, Pike RM. Survey of laboratory-acquired infections. Am J Pub Health 1951; 41:769-781. [ Links ]
61. van den Ende M, Stuart-Harris CH, Harries HER, Steigman AJ. Laboratory infection with murine typhus. Lancet 1943; 1:328-332. [ Links ]
62. Topping NH. Typhus fever. A note on the severity of the disease among unvaccinated and vaccinated laboratory personnel at the National Institute of Health. Am J Trop Med 1944; 24:57-62. [ Links ]
63. van den Ende M, Hargreaves WH, Locket S, Niven J. Accidental laboratory infection with tsutsugamushi rickettsia. Lancet 1946; 2:4-7. [ Links ]
64. Sleisenger MH, Murray ES, Cohen S. Rickettsialpox case due to laboratory infection. Pub Health Rep 1951; 66:311-316. [ Links ]
65. Johnson JE III, Kadull PJ. Laboratory-acquired Q fever. A report of fifty cases. Am J Med 1966; 41:391-403. [ Links ]
66. Bellanca J, Iannin P, Hamory B, Miner WF, Salaki J Stek M. Laboratory-acquired endemic typhus—Maryland. MMWR 1978; 26:215-216. [ Links ]
67. Becah Y, Socolovschi C, Raoult D. Identification of rickettsial infections by using cutaneous swab specimens and PCR. Emerging Infect Dis 2011; 17:83-86. [ Links ]
68. Harden VA.
69. Hazard PB, McCroan JE.
70. Johnson JE III, Kadull PJ.
71. Oster CN, Burke DS, Kenyon RH, Ascher MS, Harber P, Pedersen CE. Laboratory-acquired Rocky Mountain spotted fever. The hazard of aerosol transmission. N. Engl J Med 1977; 297:859-863. [ Links ]
72. Chosewood LC,
73. Sejvar JJ, Johnson D, Popovic T, Miller JM, Downes F, Somsel P, et al. Assessing the risk of laboratory-acquired meningococcal disease. J Clin Microbiol 2005; 43:4811-4814. [ Links ]
74. Department of Health and Human Services. Possession, use and transfer of select agents and toxins; biennial review; final rule. Fed Reg 2012; 77:61084-61115. [ Links ]
75. McDade JE. Diagnosis of rickettsial diseases—a perspective. Eur J Epidemiol 1991; 7:270-275. [ Links ]
76. Bustamente Moreno JG, Pon Méndez A. Actualización en la vigilancia epidemiológica de “rickettsiosis”. Part I. Epidemiológia Boletin 2010; 6:1-4. [ Links ]
77. Demma LJ, Traeger MS, Nicholson WL, Paddock CD, Blau DM, Eremeeva ME, et al. Rocky Mountain spotted fever from an unexpected tick vector in
78. Karpathy SE,
79. Eremeeva ME, Zambrano ML, Anaya L, Beati L, Karpathy SE, Santos-Silva MM, et al. Rickettsia rickettsii in Rhipicephalus ticks,
80. de Sousa, R, França A, Nòbrega SD, Belo A, Amaro M, Abreu T, et al. Host- and microbe-related risk factors for and pathophysiology of fatal Rickettsia conorii infection in Portuguese patients. J Infect Dis 2008: 198:576-585. [ Links ]
81. Liddell AM, Sumner JW, Paddock CD, Rikihisa Y, Unver A, Buller RS, et al. Reinfection with Ehrlichia chaffeensis in a liver transplant recipient. Clin Infect Dis 2002; 34:1644-1647. [ Links ]
82. Stenos J, Graves SR,
83. Singhsilarak T, Leowattana W, Looareesuwan S, Wongchotigul V, Jiang J, Richards AL, et al. Short report: detection of Orientia tsutsugamushi in clinical samples by quantitative real-time polymerase chain reaction. Am J Trop Med Hyg 2005; 72:640-641. [ Links ]
84. Paris DH,
85. Renvoisé A, Rolain JM, Socolovschi C, Raoult D. Widespread use of real-time PCR for rickettsial diagnosis. FEMS Immunol Med Microbiol 2012; 64:126-129. [ Links ]
86. Kato CY, Chung IH, Robinson LK, Austin AL,
87. Buller RS, Arens M, Hmiel SP, Paddock CD, Sumner JW, Rikihisa Y, et al. Ehrlichia ewingii, a newly recognized agent of human ehrlichiosis. N Engl J Med 1999; 341:148-155. [ Links ]
88. Balcells, ME, Rabagliati R, Garcia P, Poggi H, Oddó D, Concha M, et al. Endemic scrub-typhus-like illness, Chile. Emerging Infect Dis 2011; 17:1659-1663. [ Links ]
89. Leitner M, Yitzhaki S, Rzotkiewicz S, Keysary A. Polymerase chain reaction-based diagnosis of Mediterranean spotted fever in serum and tissue samples. Am J Trop Med Hyg 2002; 67:166-169. [ Links ]
90. Jiang J, Sangkasuwan V, Lerdthusnee K, Sukwit S, Chenchitra T, Rozmajzl PJ. Human infection with Rickettsia honei,
91. Murphy H, Renvoisé A, Pandey P, Parola P, Raoult D. Rickettsia honei infection in human, Nepal, 2009. Emerg Infect Dis 2011; 17:1865-1867. [ Links ]
92. Socolovschi C, Mediannikov O, Sokhna C, Tall A, Diatta G, Bassene H, et al. Rickettsia felis-associated uneruptive fever, Senegal. Emerging Infect Dis 2010; 16: 1140-1142. [ Links ]
93. Richards AL, Jiang J, Omulo S, Dare R, Abdirahman K, Ali A, et al. Human infection with Rickettsia felis, Kenya. Emerging Infect Dis 2010; 16:1081-1086. [ Links ]
94. Rozental T, Eremeeva ME, Paddock CD, Zaki SR, Dasch GA, Lemos ERS. Fatal case of Brazilian spotted fever confirmed by immunohistochemical staining and sequencing methods on fixed tissues. Ann NY Acad Sci 2006; 1078:257-259. [ Links ]
95. Zavala-Castro JE, Zavala-Velázquez JE, Walker DH, Ruiz Arcila EE, Laviada-Molina H, Olano JP, et al. Fatal human infection with Rickettsia rickettsii, Yucatán, Mexico. Emerging Infect Dis 2006; 12:672-674. [ Links ]
96. Cragun WC, Barlett BL, Ellis MW,
97. Shapiro MR, Fritz CL, Tait K, Paddock CD, Nicholson WL, Abramowicz KF, et al. Rickettsia 364D: a newly recognized cause of eschar-associated illness in California. 2010; 50:541-548. [ Links ]
98. Wang JM, Hudson BJ, Watts MR, Karagiannis T, Fisher NJ, Anderson C, et al. Diagnosis of Queensland tick typhus and African tick bite fever by PCR of lesion swabs. Emerging Infect Dis 2009; 15:963-965. [ Links ]
99. Socolovschi C, Renvoisé A, Brouqui P, Parola P, Raoult D. The use of eschar swabs for the diagnosis of African tick bite fever. Ticks and Tick-borne Dis 2012; 3:360-362. [ Links ]
100. Mouffok N, Socolovschi C, Benabdellah A, Renvoisé A, Parola P, Raoult D. Diagnosis of rickettsioses from eschar swab samples,
101. Myers T, Lalani T, Dent M, Jiang J,
102. Johnston SH, Glaser CA, Padgett K, Wadford DA, Espinosa A, Espinosa N, et al. Rickettsia sp. 364D causing a cluster of eschar-associated illness, California. Pediatr Infect Dis J 2013 (in press). Doi: 10.1097/INF.0b013e318296b24b
103. Lee SH, Kim DM, Cho YS, Yoon SH, Shim SK. Usefulness of eschar PCR for diagnosis of scrub typhus. J Clin Microbiol 2006; 44:1169-1171. [ Links ]
104. Paddock CD, Koss T, Eremeeva ME,
105. Ndip LM, Labruna M, Ndip N,
106. Zavala-Velaquez JE, Yu XJ, Walker DH. Unrecognized spotted fever group rickettsiosis masquerading as dengue fever in
107. Hildago ML, Orejuela L, Fuya P, Carrillo P, Hernandez J, Parra E, et al.
108. Romer Y, Seijo AC, Crudo F, Nicholson WL, Varela-Stokes A, Lash RR, et al. Rickettsia parkeri rickettsiosis, Argentina. Emerging Infect Dis 2011; 17:1169-1173. [ Links ]
109. Parola P, Paddock CD, Socolovschi C,
110. Phongmany S, Rolain JM, Phetsouvanh R, Blacksell SD, Soukkhaseum V, Rasachack B, et al. Rickettsial infections and fever, Vientiane, Laos. Emerging Infect Dis 2006; 12:256-262. [ Links ]
111. Reller ME, Bodinayake C, Nagahwatte A, Devasiri V, Kodikara-Arachichi W, Strouse JJ, et al. Unsuspected rickettsioses among patients with acute febrile illnesses, Sri Lanka, 2007. Emerging Infect Dis 2012; 18:825-829. [ Links ]
112. Maina AN, Knobel DL, Jiang J, Halliday J, Feikin DR, Cleaveland S, et al. Rickettsia felis infection in febrile patients, Western Kenya, 2007-2010. Emerging Infect Dis 2012; 18:328-331. [ Links ]
113. Schoeler GB, Morón C, Richards
114. Mokrani K, Tebbal S, Raoult D,
115. Prakash JAJ, Lal TS, Rosemol V, Verghese VP, Pulimood SA, Reller ME, et al. Molecular detection and analysis of spotted fever group Rickettsia in patients with fever and rash at a tertiary care centre in Tamil Nadu, India. Pathog Glob Health 2012; 106:40-45. [ Links ]
116. Pijper A, Crocker CG. Rickettsioses of
117. Pritt BS, Sloan LM, Hoang Johnson DK, Munderloh UG, Paskewitz SM, McElroy KM, et al. Emergence of a new pathogenic Ehrlichia species, Wisconsin and Minnesota, 2009. N Engl J Med 2011; 365:422-429. [ Links ]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}