










Servicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkActa Médica Costarricense
versión On-line ISSN 0001-6002versión impresa ISSN 0001-6012
Acta méd. costarric vol.55 no.3 San José jul./sep. 2013
Original
Waist
circumference as indicator of cardiovascular risk
Ana Gladys Aráuz-Hernández, Sonia
Guzmán-Padilla,
Marlene Roselló-Araya
Study made in Área de Salud de Santa Ana
Author’s
affiliation:
Abstract
Background:
Obesity
affects more that 60% of Costa Rican adults. There is consensus on the
fact
that fat accumulation in the intra-abdominal region is a risk for
cardiovascular disease, and that the measurement of waist circumference
is an
indirect indicator used for its identification.
The
objective of the present study was to use this
measurement to describe the characteristics of the urban population and
its
stratification according to the risk level of suffering cardiovascular
diseases.
Methods: The study´s population consisted of 325 adults
(76.9%
women), ages between 20 and 44 years old; residents of the Santa Ana
Health
Area, which were at home at the time of the regular visit of the
primary health
care technician.
Results: Average
age was 30±6.5 years; 50.1% were housewives and 40.9% had elementary
schooling. The mean of the waist circumference among women was 86.4±
Conclusion:
The
structure at the primary level allows measuring the waist circumference
at
home, as a simple and practical method to identify the population at
risk.
Keywords: Waist
obesity, waist circumference, Primary Health Care, cardiovascular
diseases.
Another
reason is the deregulation in the production
of cytokines, due to fat excess, that increases a state of chronic
inflammation
that leads to insulin resistance.13 There
is a consensus about waist circumference measurement as a indirect
indicator of
presence of intraabdominal fat. It’s easy
to
obtain and have a low cost, sue to this, it is used to predict early
the risk
of diseases such as diabetes mellitus, hypertension and cardiovascular
diseases, and provides useful information to identify the risk
population, even
before the obesity is identify with BMI (Body Mass Index).14,15 However,
for this measurement to be useful and reliable, it is necessary the
existence
of measurement and standardization protocols to the staff that
performed this
measurements, in order to avoid errors that could affect the risk
classification with the obtained data.16
There are
various criteria to evaluate the risk of
cardiovascular diseases, in relation to the value of abdominal
circumference;
the Adult Panel Treatment III (APT-III) established a values of ≥80cm
in
women and ≥94cm in men, to define abdominal obesity or incremented risk.9,17,18
The International Diabetes Federation (IDF) established values of
≥90cm
in men and ≥80cm in women.19 In 1997, World Health
Organization (WHO) proposed cut points to identify people in risk into
three
categories, “very low” ≤79cm in women and ≤93cm in men;
“incremented risk” from 80 to 87cm in women and from 94 to 101cm in
men, and “high risk” ≥
In Costa
Rica, the indication for measurement of waist
circumference is establish in guides for the attention of diabetic and
hypertensive individuals.21 However, it is not considered
as a
primary care activity in Basic Health Care Crew (Equipos
Básicos de Atención
en Salud -EBAIS), with an essential
function in
health promotion and disease prevention. Each EBAIS is composed of a
doctor, a
nurse and a primary health care technician (ATAP); distributed over the
country
and attends from 3500 to 5000 habitants each.21 Due to
this, an
opportunity was identify to include the measurement of waist
circumference in
daily routine activities of ATAP’s during
home
visits, in order to identify the population in risk and refer them to
local
interventions in health prevention and promotion.
The
objective of this article is to describe the
characteristics of the population in Santa Ana Health Care Area, to
whom the
waist circumference were taken and stratification according to the risk
of
cardiovascular diseases was made.
Methodology
Cross-section
descriptive studies made in January 2009
and December
ATAP’s
were trained and standardized in the process of measurement based on
“manual de procedimiento para
la medición de la circunferencia
abdominal” (Waist circumference measurement procedure manual), designed
with this purpose.21 Fiberglass, inextensible measurement
tapes,
graduated in centimeters, and sensible to millimeters, calibrated by
Costa
Rican Measurements Laboratory (LACOMET, certified number 22010109).
The
analyzed variables were: age in years, genre,
level of schooling, occupation and waist circumference; and WHO
classification
was used.20 The occupation of remunerated activities were
classified
according to the International Labour
Organization
(ILO).23 Descriptive statistics and the analysis of the
association
of different variables with the level of risk were made with SPSS
program, ver.
15.0 for Windows. The level of statistical significance was of p<0,05.
Results
The
results of 325 people, 76,9%
were women, with an average age of 30±6,5 years, similar in both genre.
74,2% of the population were under 35 years
old. According to
the level of schooling, 40,9% of the
population had
primary education (complete or incomplete), 46,1% had middle education
(complete
or incomplete), 11,1% had college studies and 1,8% were illiterate. 50,1% were housewives, and 47,7% had remunerated
activities,
mainly services, commerce, operator workers and artisans; 72,6% of the
population were married or live in cohabitation.
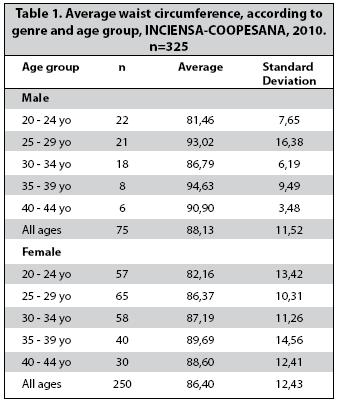
The
average waist circumference measurement in women
was of 86,4±12,4cm, and of 88,1±11,5cm
in men. There was no statistical significance between waist
circumference means
by genre (p=0,282). There was an increase of waist circumference in
women
according to age, up to 39 years old, with and statistical significant
differences (p= 0,03); in men, there was no ascendant change in age
groups, but
it was statistically significant (p=0,04). (Table 1).
{kind=link}
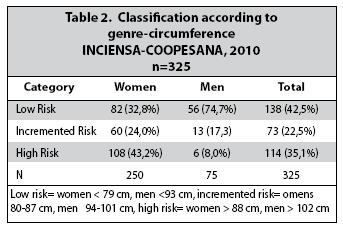
According
to WHO cut points, 57,5%
(n=187), the population was classified with some risk degree
(intermediate and
high risks). From these percentage, 35,1%
with high
risks (43,2% women and 8% men) (Table 2).
{kind=link}
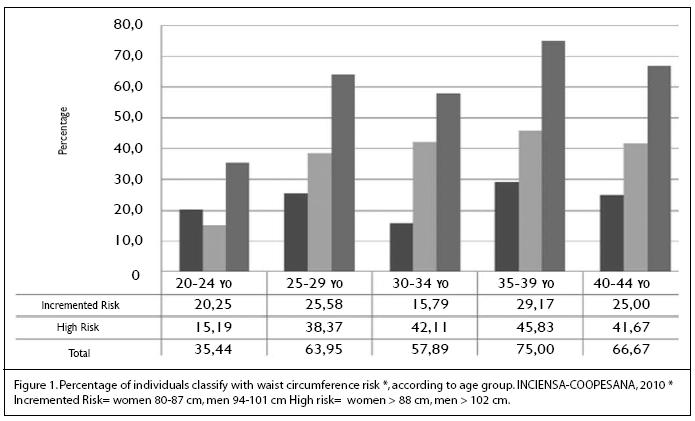
The
percentage of population in “high
risk” category had increase in each age group especially in women,
however, the major change in prevalence was in age group between 20-24
years
old and 25-29 years old (Figure 1). In men,
the most prevalent age group accounting
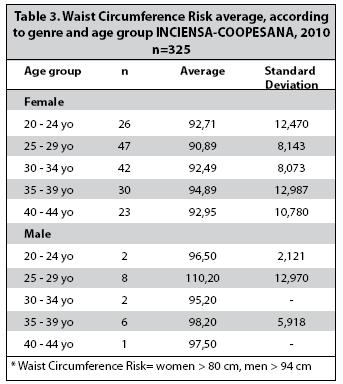
for 85% (n=5) was that of ages 35-39. Excluding low risk individuals,
an
average waist circumference in women in all age groups was over 88cm
and in
men, only age group between 25-29 years old were over 102cm, placing
them in
high risk category (Table
3).
{kind=link}
{kind=link}
Discussion
Waist
circumference is a easy
to determine tool and of great use in clinical practice, and as a
product of
study, the measurement of the waist circumference was included in
health
promotion and prevention in primary care attention.
The
population in this study was characterized with a
majority of individuals being young women, with level of schooling no
higher
than middle school, and housewives, indicators of low socioeconomically
status.
Also, the waist circumference placed them in risk of diseases such as
diabetes
and hypertension; the results on other studies indicate that obesity
problems
is a higher and more accentuated in low socioeconomically status.24,
25
The profile of individuals in this study, in addition to high values of
waist
circumference, can explain the high prevalence of diabetes in women in
Costa
Rica, shown in national surveys.3, 4
A survey
of “diabetes, hypertension and risk
factors for chronic diseases” performed in 2004, used WHO waist
circumference risk factors values, that showed a group with ages
between 20-39,
and a prevalence of 44,8% in women and 17% in men.3,
International
organizations (APT, ADF and WHO) use
different criteria to classify population in risk, concurring with the
cut
point of 80cm in women, but not in men. Many authors recommend
reevaluate the
cut values of 102cm in men, in order to avoid lately interventions; so
that in
this study 19 more men could be classify in the risk category according
to IDF.
9,27
One
limitation in these results is that the type of
population were found in households were not representative of the
general
population, since visiting hours were made in the morning, family
members that
were not at home were especially men. The limitation were for all
activities in
home visits, therefore other strategies must be sought to capture this
population, and a possible site would be the local job centers.
In
conclusion, this indicator is practical, non
invasive, and accepted by all users and health care givers, and it can
be used
in prevention at community level;28
it
allowed the identification of population in risk, that due to a younger
age
were not in demand for cardiovascular diseases, but could be include in
local
interventions in health promotion and prevention in primary care
attention.
Acknowlegments:
to the staff of COOPESANA R.L. (Santa Ana Health Corporation),
especially to ATAP’s that recollected all
data. To
Dr. Hilda Núñez Rivas for her technical
support in this project.
References
1. Barquera S, Campos I, Hernández L, Flores M, Durazno R, Kanter R, et al. Obesity and central adiposity in Mexican adults: results from the Mexican National Health and Nutrition Survey. Salud Pública Méx 2006; 51:595-603. [ Links ]
2. Ministerio de Salud. Memoria institucional 2011. San José Costa Rica: Ministerio de Salud, 2011. Recuperado el 14 de julio de 2010. En: http://www.ministeriodesalud.go.cr/ sobre_ministerio/memorias/memoria2012/UMI_memoria_ institucional_2011. [ Links ]
3. Ministerio de Salud. Encuesta Nacional de Nutrición 2008-2009. Antropometría. San José, Costa Rica: Ministerio de Salud, 2009. (monografía en línea). Recuperado el 14 de julio de 2010. En: http://www.ministeriodesalud.go.cr/index.php/component/ content/article/43-pagina-inicio-ms/145-estadiscticas-encuestasms. [ Links ]
4. Ministerio de Salud. Encuesta multinacional de diabetes mellitus, hipertensión arterial y factores de riesgo asociados área metropolitana. San José, Costa Rica: Ministerio de Salud, 2004. (monografía en línea). Recuperado el 14 de julio de 2010. En: http://www.ministeriodesalud.go.cr/index.php/component/ content/article/43-pagina-inicio-ms/145-estadiscticas-encuestas-ms. [ Links ]
5. Calle E, Thun M, Petrelli J, Rodriguez C, Heath C. Body-mass index and mortality in a prospective cohort of U.S. adults. N Engl J Med 1999; 341:1097-1105. [ Links ]
6. Klein S, Allison D, Heymsfield S, Kelley D, Leibel R, Nonas C, et al. Waist circumference and cardio metabolic risk: a consensus statement from shaping americas´s health: association for weight management and obesity prevention. Am J Clin Nutr 2007; 85:1197-202. [ Links ]
7. Benetou V, Bamia C, Trichopulos D, Mountokalakis T, Psaltopoulous T, Trichopolou A. The association of body mass index and waist circumference with blood pressure depends on age and gender: a study of 10,928 non-smoking adults in the Greek EPIC cohort. Eur J Epidemiol 2004; 19:803-804. [ Links ]
8. Lemieux S, Prud´homme D, Nadeau A, Tremblay A, Bouchard C, Després J. Seven-year changes in body fat and visceral adipose tissue in women. Association with indexes of plasma glucose-insulin homeostasis. Diabetes Care 1996; 19:983-991. [ Links ]
9. Wang Y. Rimm E, Stampfer M, Willet W, Hu F. Comparison of abdominal adiposity and overall obesity in predicting risk o type 2 diabetes among men. Am J Clin Nutr 2005; 88; 555-563. [ Links ]
10. Kisse bah A, Freedman D, Peiris A. Health risks of obesity. Med Clin North Am 1989; 73:111-138. [ Links ]
11. Ledoux M, Lambert J, Reeder B, Despres J. Correlation between cardiovascular disease risk factors and simple anthropometric measures. Canadian Heart Health Survey Research group. Can Med Assoc J 1997; 157(suppl 1):S46-53. [ Links ]
12. Wang J, Thornton J, Bari S, Williamson B, Gallagher D, Heymsfield S, et al. Comparisons of waist circumferences measured at 4 sites. Am J Clin Nutr 2003; 77:379-84. [ Links ]
13. Ramones I, Hernández R. Rol de las citoquinas en la fisiopatología del daño vascular en la obesidad. (Revista en internet) 2012. Recuperado el 23 de abril del 2013; XXVI: (aprox. 4p). Disponible en http://bibmed.ucla.edu.ve/db/psm_ucla/edocs/BM260104/BM26010408.pdf. [ Links ]
14. Pouliot M, Després J, Lemieux S, Moorjani S, Bouchard C, Tremblay A, et al. Waist circumference and abdominal sagittal diameter: Best simple anthropometric indexes of abdominal visceral adipose tissue accumulation and related cardiovascular risk in men and women. Am J Cardiol 1994;73:460-468. [ Links ]
15. Zhu S, Heshka S, Wang Z, Shen W, Allison D, Ross R, et al. Combination of BMI and waist circumference for identifying cardiovascular risk factor in whites. Obes Res 2004; 12:633-645. [ Links ]
16. Seidell J, Kahn H, Williamson D, Lissner L, Valdez R. Report from a Centers for Disease Control and prevention Workshop on use of adult Anthropometry for public health and primary health care. Am J Clin Nutr 2001; 73:123-126. [ Links ]
17. Clinical guidelines on the identification, evaluation and treatment of overweight and obesity in adults. The evidence report. National Institutes of Health. Obes Res 1998; 6(suppl 2):51S-209S. [ Links ]
18. Third Report of the National Cholesterol Education Program (NCEP) Expert panel on detection, evaluation, and treatment of high blood cholesterol in adults. (Adult Treatment Panel III). Final Report. Circulation 2002; 106; 3143-3421. [ Links ]
19. Alberti K, Zimmet P, Shaw J. The metabolic syndrome a new worldwide definition. Lancet 2005; 366(9491):1059-1062. [ Links ]
20. World Health Organization. Obesity, preventing and managing the global epidemic-report of a WHO consultation on obesity. Geneva: WHO. 1997. [ Links ]
21. Ayala N, Carvajal X, Fonseca J, Guzmán A, Marín F. Hacia un nuevo modelo de atención integral de salud. San José, Costa Rica: Caja Costarricense de Seguro Social, 1998. pág 21. [ Links ]
22. Guzmán S, Aráuz AG, Roselló M, Núñez H. 2009. Manual de procedimiento para la medición de la circunferencia abdominal. En; http://www.inciensa.sa.cr/files/refs/cvsp/medicion_ abdominal.pdf. [ Links ]
23. Resolución sobre la actualización de la clasificación internacional uniforme de ocupaciones (monografía en línea). En: http:// unstats.un.org/unsd/statcom/doc08/BG-ISCO-08-S.pdf. Stevens J, Katz E, Huxley R. Associations between gender, age and waist circumference. Eur J Clin Nutr 2010.64:6-15. [ Links ]
24. Lemieux S, Prud´homme D, Nadeau A, Tremblay A, Bouchard C, Després J. Anthropometric correlates to changes in visceral adipose tissue over 7 years in women. Int J Obes 1996; 20:618-624. [ Links ]
25. Zuzunaga A, Villarreal J. Índice cintura-cadera y perímetro abdominal: su relación con la hipertensión arterial y la diabetes mellitus en una población femenina. Rev Soc Perú Med Interna (publicación periódica on line) 2002; 15(3):129-133. En:
26. The Emerging Risk Factors Collaboration. Separate and combined associations of body-mass index and abdominal adiposity with cardiovascular disease: collaborative analysis of 58 prospective studies. Lancet 2011; 377:1085-1095. [ Links ]
27. Balkau B, Deanfield J, Després J. Bassand J, Fox K, Smith S, Barter P, et al. International day for the evaluation of abdominal obesity (IDEA). Circulation. (publicación periódica on line) 2007; 116: 1942-1951. En: http://circ.ahajournals.org Recuperado el 20 de mayo de 2008. [ Links ]
 Todo el contenido de esta revista, excepto dónde está identificado, está bajo una Licencia Creative Commons
Todo el contenido de esta revista, excepto dónde está identificado, está bajo una Licencia Creative Commons

actamedica@medicos.cr