










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkActa Médica Costarricense
On-line version ISSN 0001-6002Print version ISSN 0001-6012
Acta méd. costarric vol.55 n.3 San José Jul./Sep. 2013
Original
Original
Surgical treatment of fecal incontinence
Norma Ceciliano-Romero y
Silvia Cordero-Castro
Work performed at the Department of General Surgery, National Children’s Hospital “Dr. Carlos Sáenz Herrera”. * nocerodd@hotmail.com Support sources: no financial aid was available.
Resumen
Background: Patients with fecal
incontinence suffer
from serious social and psychological problems. Therefore, the
objective was to
analyze the evolution of 27 patients who underwent surgery using the
Malone,
Neo-Malone or Chait’s Button procedures in
order to administer an antegrade enema.
Also, the
study aimed at assessing the effect of performing the procedure on
their
quality of life.
Methods: Research is descriptive and
retrospective. Data
was obtained from medical records from the period 2000-
Results: Out of the 27 patients analysed,
an anorectal deformity was the cause of
incontinence
in 21, mielomeningocelein 3, Hirschsprung
disease in 1, rabdomiosarcoma in 1 and
constipation
in 1. The Malone procedure was used in 17 of these patients, the
Neo-Malone in
6 and the Chait’s Button in 4. The
complications
observed were: leakage from the neo-appendix with peritonitis and
reoperation
in 1 case, stenosis of the stoma in 9
cases, granulomas in 4 cases and prolapse
in 1 case. In 24 cases, patients keep clean from feces and both,
patients and
parents are satisfied. In 10 cases, patients are independent and
administer
their own enemas.
Conclusions: The results allow us to
consider that
surgery to administer an antegrade enema
is a good
alternative to improve the patient´s
quality of
life.
Keywords: Malone, Neo-malone,
Chait’s Button, fecal incontinence.
The
problem of fecal incontinence is very severe for
the child who suffers from it and their families. It is considered that
75% of
patients who are born with anorectal
malformation,
with current treatments, can be able to have a good fecal continence.
The
remaining 25% are incontinent.1 There
are
also other conditions such as myelomeningocele,
which
also leave patients incontinent. Sequels that this problem presents are
important psychological disorders, school dropouts, family dysfunction
and
social disapproval. To try and correct these problems the
colorectal
disorders Clinic was created, where 27 patients has been
controlled
undergoing the following procedures: Malone and neo-appendix, which are
two
different techniques to treat the problem in the first one, using the cecal appendix, and the second one, with a duct
of the
colon wall. (Figure 1),
which have a particular relationship to the skin, which
allows to perform cleansing enemas inversely to the traditional or in
the same
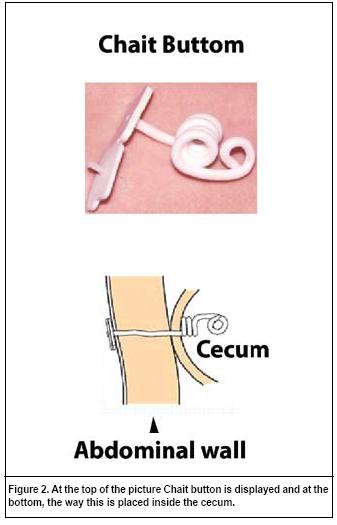
direction of the bowel movements. This is what has been called antegrade enemas. In some patients the Chait’s
button was inserted, a plastic device used to communicate the large
intestine
in its antimesenteric border with the skin
at the
front of the abdomen, usually placed on the right side. (Figure 2)
The
objective of this research was to analyze patients
treated with the three techniques.
Methods
It is a
descriptive study, with retrospective
direction, and to collect clinical data, clinical files were used that
included
the postoperative follow-ups during consultation. Some information was
necessary to complete by telephone, when patients lived in remote rural
areas.
In all
patients before undergoing surgery, a careful research
was performed on: a) if they had an appendix and whether it could be
used, or
if because of a previous surgery, the existence of many adhesions was
suspected, b) if patients understood the procedure and if they agreed
to it, c)
if the family understood and agreed to the procedure. The patients that
underwent an appendectomy were also given a choice between the
neo-appendix and
the Chait’s button.
To select
the patients the following parameters were
used: a) their fecal incontinence had not responded to medical
treatment, b)
that they would have had any of the three surgical procedures as
described.
The study
was conducted in the period between 2000 and
2010. Variables were analyzed, such as the cause of the fecal
incontinence, the
type of surgical procedure performed (Malone, Neo-appendix, Chait’s
button)2 and if it
was performed
with open or laparoscopic surgery. Complications that were presented in
each of
the procedures are also analyzed. Finally, the results were analyzed,
assessing
if the patient was kept clean, if they were able to perform the enemas
on their
own, and what their and their family’s level of satisfaction was.
This
research was presented and approved by the
Institutional Bioethics Committee at the 016-2011 session.
Results
27
patients were studied, 12 female and 15 male. Their
age was between 4 years the youngest and 17 the oldest, with a mean of
10 and a
mode of 9.
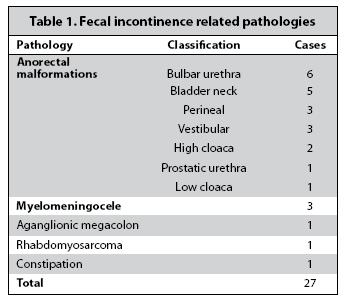
The
pathology that led to incontinence is shown in (Table
1). The surgery performed consisted of 18 procedures performed with
open
surgery, where a laparotomy was performed
and 9
underwent the laparoscopic technique. The Malone technique was
performed on 17,
the neo-appendix on 6 and the placement of a Chait’s
button on 4.
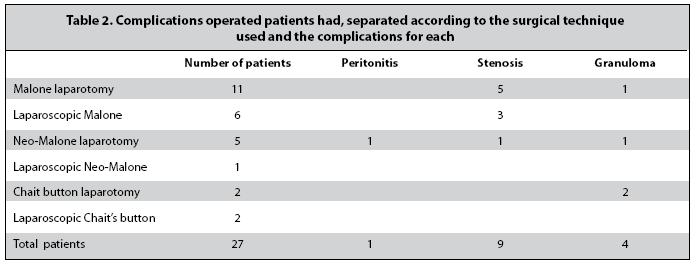
The
complications presented are analyzed in Table 2. The
only complication of peritonitis was in one case of neoappendix,
and granuloma was more common when the Chait’s button was used.
In 24
cases it was possible to keep the patient clean,
using one or two enemas a day (88.88%). In 10 of the latter cases the
fact that
they were independent was accomplished, that they themselves performed
the antegrade enema (41,66
%).
Patients
that were kept clean were found satisfied
with the procedure as well as their families.
Discussion
Patients
with anorectal
malformations who had perineal and
vestibular
fistulas, where they should get good results with the surgery, showed
malformations in the spine and their sacral index was very low. This
has been
the cause of incontinence, which has been reported in the bibliography.1,3
When the
Malone or Neo Malone procedure was performed,4,5
the outlet of the duct was
attempted to be placed in the umbilical scar for aesthetic reasons and
to not
interfere with concomitant urologic procedures, since some of these
patients
also deserve urinary system surgery.6,7 When Chait’s
button was inserted,8 the cecum
was used
and this was located on the right side of the abdomen.
The most
common complication was mouth stenosis,
which was treated with dilations and in three
cases the Chait’s button was placed in for
a
while, and when removed dilations were continued, technically,
modification of
the technique was described to avoid this type of complication.9 Granulomas were treated with applications of
sodium
chloride or mercurochrome. Mucosa prolapse
required a
reoperation for correction. In order to prevent leakage of intestinal
contents
into the cavity and subsequent peritonitis, the cecum
is attached to the abdominal wall.
The small
number of patients does not allow for
conclusions that have a statistical value, and only seems to indicate
that the
Malone technique yields an increased number of stenosis
and the use of laparoscopic techniques does not increase complications,
regarding surgical interventions performed for antegrade
enemas, they are considered a good option to improve their quality of
life. The
existence of a multidisciplinary team for management is required.
Studying the
problem must be continued to achieve higher data and, in particular, to
learn
its development in adulthood.
Conflicts
of interest: from both authors, there are no
conflicts of interest.
Referencias
1. Peña A, Hong A. Advances in the Management of Anorectal Malformations. Am J Surg 2000; 180:370-376. [ Links ]
2. Peña M, Parés D, Pascual M, Pérez M, Cañete N, Sánchez M, Andréub M, Grande L. Tratamiento del estreñimiento crónico grave mediante la técnica del enema anterógrado continenete. Cir Esp 2008; 80: 403-405. [ Links ]
3. Peña A, Guardino K, Tovilla J, Levitt M, Rodríguez G, Torres R. Bowel Management for Fecal Incontinence in Patients with Anorectal Malformations. J Pediatr Surg 1998; 33:133-137. [ Links ]
4. Levitt A, Soffer S, Peña A. Continent appendicostomy in the bowel management of fecally incontinent children. J Pediatr Surg 1997; 32:1630-1633. [ Links ]
5. Weiser A, Stock J, Hanna M. Modified cecal flap noeappendix for Malone antegrade continence enema procedure: a novel technique. J Pediatr Urol 2003; 169: 2321-2324. [ Links ]
6. Meurette G, Lehur P, Coron E, Regenet N. Long-term results of malone´s procedure with antegrade irrigaton for severe choronic constipation. Gastroenterol Clin Biol 2010; 34:209-212. [ Links ]
7. Bau MO, Younes S, Aupy A, Bernuy M, Rouffet MJ, Yepremian D, Lottman HB. The Malone antegrade colonic enema isolated or associated with urological inconticence procedueres: evaluation from patient point of view. J Pediatr Urol 2001; 165: 2399-2403. [ Links ]
8. Becmeur F, Demarche M, Lacreuse I, Molinaro F, Kauffmann I, Moog R, et al. Cecostomy button for antegrade enemas: survey of 29 patients. J Pediatr Surg 2008; 43: 1853-1857. [ Links ]
9. Shaul DB, Harrison EA, Muenchow SK Avoidance of leakage and strictures when creatinag an invisible conduit for anterograde colinic enemas. J Pediatr Surg 2002; 37: 12, 1768-1771. [ Links ]


{kind=link}
{kind=link}
{kind=link}
{kind=link}