










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkActa Médica Costarricense
On-line version ISSN 0001-6002Print version ISSN 0001-6012
Acta méd. costarric vol.55 n.2 San José Apr./Jun. 2013
Caso clínico
Airway
pressure release ventilation in newborns
Enmanuel Jiménez-Castro,
Olman Coronado-García,
Leonardo Orozco-Saborío y Alicia Boza-Mora
This work was done in Dr. Adolfo Carit EvaWomen’s Hospital,Neonatology Service and Clinical Investigation Unit. * loscr@yahoo.com
Abbreviations:
APRV,
Airway pressure release ventilation; FiO2, fraction of inspired oxygen;ARF,Acute Respiratory
Failure;PaCO2,arterialcarbondioxide
tension; PaO2, arterial oxygen tension; PCV, pressure controlled
ventilation;
PEEP, positive end-expiratory pressure; PIP, peak inspiratory
pressure.
Abstract
Airway
pressure release ventilation is a mechanical
ventilation method that uses a controlled positive airway pressure in
order to
maximize alveolar recruitment, with prolonged inspiratory
times, therefore allowing spontaneous breathing during both phases of
the
respiratory cycle.
The
authors describe their experience in twelve cases
of newborn patients with acute respiratory failure treated with airway
pressure
release ventilation when oxygenation did not improve with pressure
control
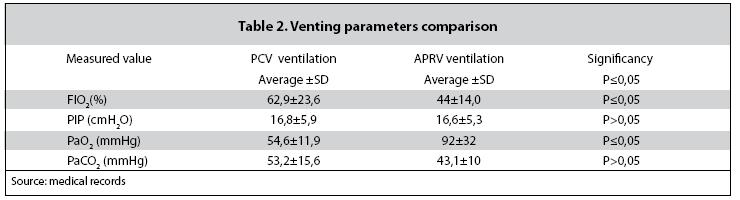
ventilation. The mean age of patients was 13 ± 16.5 days. The
fractional
concentration of oxygen (FiO2) decreased from 62.9 ± 23.6 cmH2O for
pressure control ventilation to 44 ± 14.0 cmH2O for airway pressure
release ventilation. The mean partial arterial oxygen pressure
increased from
54.6 ± 11.9 mmHg to 92 ± 32 mmHg. The mean partial carbon dioxide
pressure decreased from 53.2 ± 15.6 mmHg to 43.1 ± 10 mmHg and
the peak inspiratory pressure fell from
16.8 ±
Airway
pressure release ventilation may improve
oxygenation in pediatric patients with acute respiratory failure when
conventional mechanical ventilation fails.
Keywords: Airway
pressure release ventilation, acute respiratory failure.
Case
Report
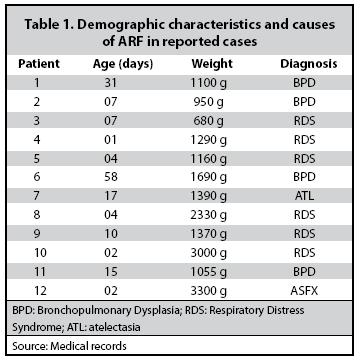
Twelve
patients that developed ARF were treated with
APRV. The underlying causes of the respiratory failure and the
demographic data
and etiology of respiratory failure are shown in Table 1.
{kind=link}
Before
applying APRV, patients were ventilated using
PCV, with sequential PIP and PEEP increments, in an attempt to achieved
maximum
oxygenation. The venting parameters prior to APRV conversion are shown
in Table
2.
{kind=link}
All the
patients were ventilated with Galileo Gold
Hamilton Medical AG (
Discussion
For data
analysis, the Cochrane Collaboration
Statistical Package, Rev Man Version 5.1 was used. The results obtained
in this
case analysis, showed how the APRV improved the oxygenation and the
alveolar
ventilation reflected in the clinical decrease in PaCO2, although this
was not
statistically significant, a PEEP can be maintain in level 0, being
this the releasing
phase or pressure drop, the point of improvement in alveolar
ventilation. Similarly,
an improvement in the PaO2 can be observe with less inspiratory
pressure and a lesser oxygen inspired fraction (FIO2), resulting in
less
pulmonary parenchyma injury, produced also by diminishing the frequency
of
changes in airway pressure of the APRV.
Demirkol
et al,3 indicated the
airway
optimization, improving the recruitment through open lung
stabilization.
Meanwhile,
in their case report, García
et al10 showed that when APRV is
used
proactively, there is an improvement in blood gas and accelerated
weaning, so
the use of this venting technique can be complemented proactively, and
not for
rescue as shown in this series.
In
different studies10-11, parameters such
as high P above 20 to 25cm H2O has been used; in the case of exposed
patients,
the average high P was 16,6cm H2O, achieving the same improvement in
oxygenation, diminishing the possible complications of barotrauma.
The
obtained PaO2 improvements in this study after placing
APRV were statistically significant with a lower FIO2, supporting the
hypothesis of open lung stabilization, which is show with a
statistically
significant decreased in FIO2 parameters, but not in PaCO2, which
showed
decreased levels after APRV mode was applied, with no statistically
significant
differences.
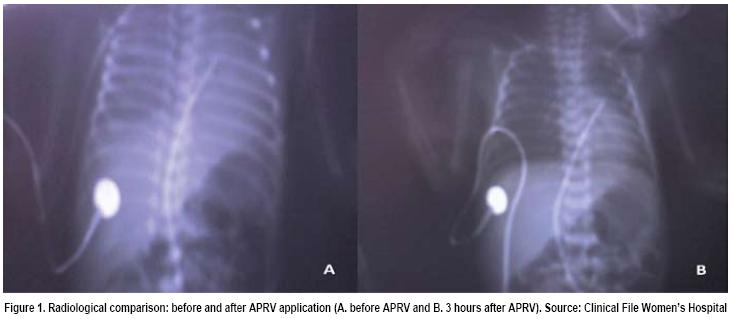
Another
advantage shown with the use of APRV is the
radiological improvement within 3 hours (Figure 1), that is
evidence
with an
improvement in the alveolar recruitment without any hemodynamic
impairment. Demirkol study refers that
APRV can offer potential clinical
advantages, and so it should be considered as an alternative modality
in
mechanic ventilation for the pediatric population3 and in
this
report the improvements on PaO2 and PaCO2 with a lower pressure and
lower FIO2
values are evidenced, being this an advantage for managing the
ventilation in
newborns with ARF.
{kind=link}
In
conclusion, the use of APRVachieved
an improvement in blood gas parameters, radiological imaging, and
contribute to
break the habit of using mechanic ventilation. In future controlled
clinical
essays, the efficacy of implementing this type of ventilation in
newborns can
be proved.
Conflict
of interests: the
authors declare no conflict of interests with the publication of the
study.
References
1. Dart BW, Maxwell RA, Richart CM, Brooks DK, Ciraulo DL, Barker DE. Preliminary experience with airway pressure release ventilation in a trauma/surgical intensive care unit. J Trauma2005; 59:71–6. [ Links ]
2. Petsinger DE, Fernandez JD, Davies JD. What is the role of airway pressure release ventilation in the management of acute lung injury Respir Care Clin 2006; 12:483–8. [ Links ]
3. Demirkol D, Karabocuoglu M, Citak A. Airway Pressure Release Ventilation: An Alternative Ventilation Mode for Pediatric Acute Hypoxemic Respiratory Failure. Indian J Pediatr 2010;77:1322– 1325. [ Links ]
4. Downs JB, Stock MC. Airway pressure release ventilation: a new concept in ventilatory support. Crit Care Med 1987; 15:459–61. [ Links ]
5. Stock MC,
7. Foland JA, Martin J, Novothy T, Super DM, Dyre RA, Mhanna MJ. Airway pressure release ventilation with a short release time in a child with acute respiratory distress syndrome. Respir Care 2001; 46:1019–23. [ Links ]
8. Krishnan J, Morrison W. Airway pressure release ventilation: a pediatric case series. PediatrPulmonol 2007; 42:83–8. [ Links ]
9. Schultz TR, Costarino AT, Durning SM. Airway pressure release ventilation in pediatrics. PediatrCrit Care Med 2001; 2:243–6. [ Links ]
10. Garcia P, Henry J, Hughes S, Boylan C. A case series of infants on APRV in the neonatal ICU. 1 página. Recuperado el 2 de junio de 2011, de http://www.rcjournal.com/ abstracts/2007/?id=aarc07_236. [ Links ]
11. Blake B, Perrette Julianne, Gilmore M. Case Study: retrospective study of using APRV in neonates with overwhelming sepsis. 1 página. Recuperado 30 de mayo de 2011, de http://www. rcjournal.com/abstracts/2005/?id=OF-05-058%20Blake. [ Links ]
 All the contents of this journal, except where otherwise noted, is licensed under a Creative Commons Attribution License
All the contents of this journal, except where otherwise noted, is licensed under a Creative Commons Attribution License

actamedica@medicos.cr