










Servicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkActa Médica Costarricense
versión On-line ISSN 0001-6002versión impresa ISSN 0001-6012
Acta méd. costarric vol.55 no.2 San José abr./jun. 2013
Original
Surgical
treatment of Hirschsprung’s disease at the
National Children’s Hospital “Dr. Carlos Saenz Herrera”
during the period 2000-2010
Fabián García-Arias1,
Norma Ceciliano-Romero2
Work performed in the General Pediatric Surgery Department. National Children’s Hospital Dr. Carlos Sáenz Herrera
Affiliation
of authors:
1Pediatric
Surgery Department,
Abbreviations:
TERPT, transanal endorectal
pull-through; NCH, National Children’s Hospital “Dr. Carlos Sáenz Herrera”.
Abstract
Background:
Hirschsprung´s
disease (congenital megacolon) is a common
cause of
lower bowel obstruction in neonates. Its main characteristic is that a
section
of the bowel is unable to relax, causing functional colonic
obstruction.
Treatment for this disease requires the resection of the abnormal bowel
segment
in order to restore the functions of the healthy part of the intestine.
The
management and its epidemiology of this disease at the National Children´s Hospital during the period 2000 to
2010
were analyzed.
Methods: observational
and retrospective study, 130 files were reviewed using Microsoft Excel
and the
JMP® statistical software.
Results: a male:
female ratio was 4:1, most cases occurred in full term babies, and the
most
common initial symptoms were abdominal distension and bilious vomiting.
In 78%
of the cases the age at which the disease occurred was less than one
month.
Among the surgical techniques used, the Duhamel technique was the most
used
(48%), followed by the transanal
pull-through
technique (35%). The most common postoperative complication for the
Duhamel
group was rectal septum (8 out of 21 cases), and enterocolitis
in the transanal pull-through group (14
out of 19
cases).
Conclusion:
the
clinical and epidemiological characteristics of the cases of Hirschsprung’s Disease analyzed are similar to
those
reported in the literature. The postoperative complications and
morbidity was
similar for both surgical techniques.
Keywords: Hirschsprung disease, colonic aganglionosis,
Congenital Megacolon.
The most
common presentation of the disease is the
location in the rectosigmoid. However,
different
parts of the colon can be affected, and also completely; part of the
small
intestine is very rarely affected.3, 4
Early
diagnosis and management avoids the potential
complications of patients with Hirschsprung’s
disease. Among the initial studies to be performed, are contrast
enemas, rectal
manometry and rectal biopsy, which
eventually
confirms the diagnosis.5-9 Disease management has evolved
over the
years from very invasive procedures performed in several stages
including three
surgeries, to minimally invasive procedures carried out in a single
surgical
intervention.10-14
The goal
of the study was to analyze and compare the
surgical techniques used in the National Children’s Hospital Dr. Carlos
Sáenz Herrera (NCH), for the treatment of
this
condition and its results in the short and medium term. In addition,
the
epidemiology of the disease was examined.
Methods
Upon
approval of the study by the institutional
bioethics committee, the medical records were reviewed as population
taking all
patients discharged from the National Children’s Hospital diagnosed
with Hirschsprung’s disease from January
2000 to December
2010.
Patients
with the diagnosis of Hirschsprung’s
disease were included during the established term, who
had undergone surgery. Cases with incomplete records and all patients
who had Hirschsprung’s disease ruled out
were excluded from
the analysis.
Records
that met the inclusion criteria were reviewed.
Epidemiological
data was analyzed, symptomatology,
compromised intestinal segment, diagnostic procedures, surgical
intervention,
postoperative complications according to surgical technique and
associations.
Microsoft
Excel was used to analyze the data,
obtaining the results and completion of the graphics.
JMP® statistical
software was used to
digitize the data of the 87 patients treated with one of the two
surgical
methods (transanal endorectal
pull-through -TERPT -or Duhamel) and a logistic regression to determine
if
there were differences in treatment effects was built.
Results
A total of
130 records were obtained in the Statistics
Service list, with discharge diagnosis of aganglionic
megacolon or Hirschsprung’s
disease. 26 records were excluded: 11 for being incomplete and 15 for
presenting positive biopsies for ganglion cells, which allowed to rule
out Hirschsprung’s disease, so that a
population of 104
patients were left who met the inclusion criteria.
A
relationship male: female ratio of 4:1 was found,
for 80 men and 24 women, and an increased incidence in infants born at
term (83
cases). Initial symptoms were analyzed and identified bloating as the
most
frequent, followed by bilious vomiting, terminal meconium
and constipation, for a 74%, 52%, 36% and 19%, respectively. At the
same time,
it showed other forms of initial presentation less often than the
previous
ones, such as oral intolerance, vomiting clear or dairy, intestinal
obstruction, intestinal perforation, jaundice, irritability, among
others.
Most cases
occurred in less than one month: 78 cases
out of 104. No difference was found between the group of one month to
six
months and that over twelve months, 11 cases diagnosed for the first
group and
10 for the second. In the group of six to twelve months only 2 cases
occurred.
Most
patients did not associate enterocolitis
while presenting symptoms of Hirschsprung’s
disease.
At the time of diagnosis, enterocolitis
was evident
only in 18 patients.
Data was
obtained from the abdominal radiograph only
in 70% of the 104 patients. In 17% a plain abdominal radiography was
not performed
and in 13% no information was provided.
The main
finding on the plain abdominal radiograph was
diffuse distension of loops in 74 cases (85%), followed by lack of
distal air
in 34 (39%), edema in between loops in 29 (33%), fluid levels in 10
(11.5%), coprostasis in 9 (10%), ground
glass appearance in 5 (6%)
and pneumoperitoneum in 4 cases (4,5 %).
Barium
enema was performed in 66 patients (63%), 29
(28%) did not undergo the procedure, for unspecified reasons on file,
and for 9
(9%) patients, it was unable to obtain information about whether or not
they
performed a barium enema, at the moment of diagnosis.
Of the 66
patients who underwent barium enema, a
transition zone was evident in 31, which corresponds to 47%. No
transition zone
was revealed in 35 patients (53%), of which 20 (30%) had undergone a
rectal
procedure such as irrigations, digital rectal exam or stimulation with
thermometer, so that it can be shown as false negatives in the barium
enema.
Of the 31
studies that the transition zone was
demonstrated, only 16 cases (52%) were correlated with the true
transition
zone, according to the final report of Pathology, it was not correlated
in 8
cases (26%), and in 7 (22%) no information was found in the record to
indicate
at what level the transition zone was observed on the barium enema
study.
The length
of the compromised intestinal segment in 12
patients was ultrashort, short in 60
cases, long in
23, and had total megacolon in 7 cases;
and in 2
cases no documentation was found for the compromised segment.
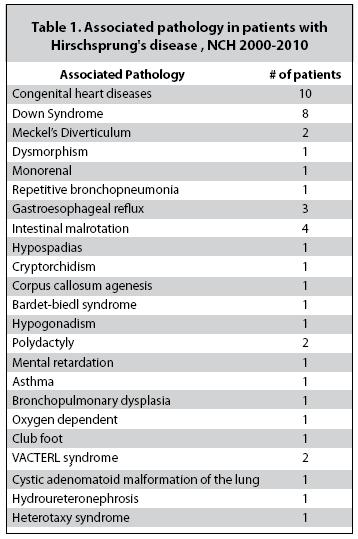
Of the 104
patients in the study, 22 showed
association with other diseases: mostly congenital heart diseases (10
patients), followed by Down syndrome (8 patients), among several
others. (Table
1)
Regarding
the type of surgery performed, the first
surgery that was performed on 48 patients was a colostomy; on 37, one
TERPT; on
13, ileostomy, and on 6, sphincter myotomy. As a final surgery for the ostomy
patients, Duhamel was conducted on 50 patients, and Soave-Boley
and Lester Martin in 1 patient each. 9 cases were documented in
patients who
have not had their definitive surgery or died without it.
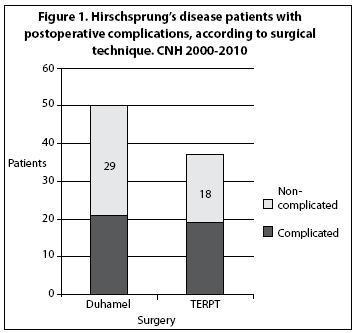
Nineteen
of the 37 patients operated on with the TERPT
technique, and 21 of the 50 patients undergoing surgery with Duhamel,
had
postoperative complications. (Figure 1)
Logistic
regression was constructed using the JPM
statistical program to determine if there are differences in treatment
effects
of the TERPT and Duhamel; the type of treatment used- TERPT and Duhamel
was
taken as dependent variable, and postoperative complications were taken
as an
independent variable. This procedure resulted in a probability
associated to
the logistic regression model of 0.30; so with a confidence level of
95% that
indicates that there is not enough evidence to affirm that there are
significant differences in the application of the above treatments.
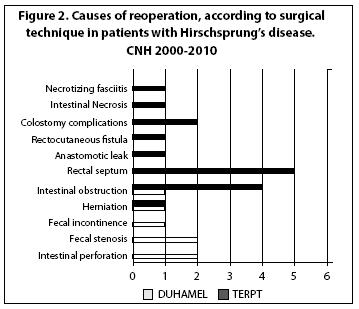
The most
common complications in the group of patients
undergoing TERPT were: enterocolitis,
rectal stenosis, constipation and
intestinal obstruction. Only 7
patients had complications that required reintervention.
(Figure 2)
In the
intervention group with the Duhamel technique,
the most common postoperative complications were: rectal septum,
intestinal
obstruction, enterocolitis and
gastrointestinal
bleeding. Among these, 16 patients required surgical reintervention.
(Figure 2)
Several
patients had more than one complication during
the postoperative follow-up period, and some may have needed surgical reintervention on more than one occasion.
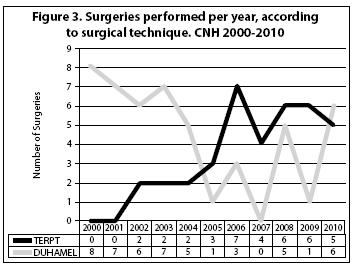
The use of
each surgical technique for both TERPT and
Duhamel was analyzed per year. (Figure 3).
Discussion
The
literature describes a predominance of Hirschsprung’s
disease in males, from 3:1 to 4:1,1,
4,15 and more frequent in term
newborns.15 In this study a relationship was found male:
female
ratio of 4:1, and 77% of the cases occurred in term newborns.
The
symptoms that were presented in order of
frequency: abdominal distension, bilious vomiting, terminal meconium
and constipation, which are correlated with that described in the
literature.4,
15,16 Most patients had symptoms
before the
first year of life and only 10% did so after the year, mainly showing
chronic
constipation, as described by various authors.17
Unlike
what is described in the literature on the
manifestation of enterocolitis the time of
diagnosis
in 50% of cases,16 in
this study
only 17% of patients had enterocolitis
when
presenting initial symptoms.
We found a
25% association with other pathologies,
slightly lower percentage than 30% found in other studies.15, 18,19
The barium
enema showed a limited value as a
diagnostic method, since only a quarter of the studies was able to
identify the
actual transition zone, which implies a lower number than found in the
literature.5, 8,9,11
The most
commonly used surgery was Duhamel procedure
in 50 of the 104 cases; the TERPT was used in 37 cases; the sphincter myotomy in 7 patients; Soave-Boley
in 1 case, and Lester Martin in another. This difference of 13 cases
between
Duhamel and TERPT could show that the TERPT began to practice in 2002,
therefore no cases were reported in the first two years during the
study; in
addition, there is no trend or pattern of use between both surgical
techniques,
during the 10 years covered.
Regarding
postoperative complications, they occurred
in 51% of the TERPT cases and 42% of Duhamnel
cases.
This is different from what was described by several authors, who
report a
higher tolerance by the child and a decreased risk of complications of
the
TERPT technique,13,14,20,21 since
there is no significant difference between the percentage of patients
who
became complicated while using both techniques.
A higher
percentage of patients requiring reoperation
were found in the TERPT group, 81%, versus 68% of the Duhamel group.
One
limitation of the study is its retrospective
design based on gathering record information, with the disadvantages
that this
confers, as no other variables were analyzed that resulted in being
interesting
to compare the results and would enrich the quality of research.
Another
limitation found was the lack of data in some cases, which prevents
analyzing
such variables.
Conflict
of Interest: There
is no conflict of interest.
References
1. Robb, A; Lander, A. Hirschsprung´s disease. Surgery (
2. Feldmon T. Wershill B. Hirschsprung Disease. Pediatr Rev.2006;27:56-57. [ Links ]
3. Martucciello G, Pini Prato A, Puri P. Controversies concerning diagnostic guidelines for anomalies of the enteric nervous system: a report from the foruth International Symposium on Hirschpring’s disease and related neurocristopathies. J Pediatr Surg 2005; 40:1527-1531. [ Links ]
4. Croaker GDH. A Cook´s tour around Hirschsprung´s disease. Current Pediatrics 2006. 16:182-191. [ Links ]
5. Diamond
6. Zaslavsky C, Baucke VL. Anorectalmanometric evaluation of children and adolescents postsurgery for Hirschsprung´s disease. . J Pediatr Surg 2003; 38:191-195. [ Links ]
7. Yunis EJ, Dibbins AW,
8. De Lorijn F, Krener LC, Ritesma JB. Diagnostic test in Hirschsprung disease: a systematic review. J Pediatr Gastroenterol Nutr 2006; 42:496-505. [ Links ]
9. Martucciello G, Pini Prato A, Puri P. Controversies concerning diagnostic guidelines for anomalies of the enteric nervous system: a report from the fourth International Symposium on Hirschpring’s disease and related neurocristopathies. J Pediat Surg 2005; 40:1527-1531. [ Links ]
10. De la Torre-Mondragón. Enfermedad de Hirschprung. Mitos y realidades a 120 años de su descripción. Acta Pediatric Mex 2008; 29: 139-146. [ Links ]
11. Peña, Alberto. Enfermedad de Hirschsprung: los avances y las preguntas no contestadas. Cir Pediatr 2002; 15: 46-47. [ Links ]
12. De la Torre-Mondragon L, Ortega-Salgado JA. Transanal versus open endorectal pull-through for Hirschprung’s disease. J Pediatr Surg 2000; 35:1630-2. [ Links ]
13. Georgeson KE, Robertson DJ. Laparoscopic-asisted approaches for the definite surery for Hirchsprung’s disease. Semin Pediatr Surg 2004; 13:256-262. [ Links ]
14. De la Torre L, Ortega Salgado JA. Transanalendorectal pull-through for Hirschoprung’s disease. J Pediatr Surg 1998; 33:1283-1286. [ Links ]
15. Kessmann J. Hirschprung’s Disease: Diagnosis and management. Am Fam Physician 2006;24:1319-1323. [ Links ]
16. Luis L.A. Encinas J. L. Enfermedad de Hirschprung: enseñanzas de los últimos 100 casos. Cir Pediatr 2006; 19:177-181. [ Links ]
17. Fantobal-Rojas A. Constipación crónica en el niño. Rol del estudio por imágenes. Revista Peruana de Radiología. 2003; 18:59-66. [ Links ]
18. De Manueles J. Enfermedad de Hirschprung. Protocolos diagnósticos y terapéuticos en pediatría. Sociedad Española de Pediatíia. Pág. 56-60. [ Links ]
19. Arriagada MP, Alfaro G, Rostion CG. Enfermedad de Hirschprung. Rev Ped Elec (en línea) 2008; 5. [ Links ]
20. Mattioli G, PiniPrato A, Giunta C, Della Roca M, Montobbio G, et al. Outcome of Primary Endorectal Pull-Through for the treatment of Classic Hirschprung’s Disease. J Laparoendosc Adv Surg Tech A 2008;18:869-874. [ Links ]
21. Pollioto S, Heinen F, Anduna G, Korman R. Evaluación del resultado a tres años de nuestra primera experiencia en el tratamiento laparoscópico de la enfermedad de Hirschprung. Cir Pediatr 2001; 14:85-87. [ Links ]


{kind=link}
{kind=link}
{kind=link}
{kind=link}