










Serviços Personalizados
Journal
Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkActa Médica Costarricense
versão On-line ISSN 0001-6002versão impressa ISSN 0001-6012
Acta méd. costarric vol.55 no.2 San José Abr./Jun. 2013
Original
Laparoscopic
nephrectomy: impact of implementation
Roy
López-Arias, Mario González-Salas
Research performed at the Urology Department,
Abbreviations:
HCG, Hospital“Dr. Rafael Ángel Calderón Guardia”;
LN, laparoscopic nephrectomy.
Abstract
Background:
The
urologic laparoscopy program started in
Methods: All the
patients who had a laparoscopic kidney procedure from 2008 to 2011 were
included. The surgical records of the laparoscopic nephrectomy
protocol were reviewed. Demographic characteristics, surgical
information,
surgical technique and approach as well as complications were analyzed.
The
histological diagnosis was reviewed in the follow up.
Results: Since
2008, 200 laparoscopic kidney procedures had been performed, including
150 nephrectomies (radical and simple), 15
pyeloplasties,
and 35 symptomatic benign cyst resections.
On
average, the neoplastic
kidney specimens weighed
Conclusion:
The
benefits from implementing the kidney laparoscopy program in our
institution
are clearly established. Variables such as less postoperative pain,
postoperative stay, patients reassuming their normal lives and
returning to
their jobs much faster compared to open surgery. Moreover, oncologic
results
are the same as in open surgery.
Keywords: Nephrectomy,
laparoscopy, kidney, surgery, urology
The
experience with laparoscopy in the Hospital
“Dr. Rafael Angel Calderon Guardia “(HCG), starts with renal cysts
and tumors confined to the kidney, which were not candidates for
partial nephrectomy because of anatomic
location. The
contraindications for laparoscopy are limited.
The
adoption of this technique of LNhas
not widespread throughout the country, mainly outside the central
hospitals,
because it is perceived as difficult, there is lack of interest in
training of
the established surgeons, lack of equipment needed for surgery, and
lack of
time on the part of surgeons to teach.
The above
is because in many cases a great number of
surgeries must be performed per day in order to reduce the waiting
lists.
This paper
describes the experience of setting the
program for LN in the
Methods
This study
included all patients who underwent a
laparoscopic procedure in the kidney in HCG from September 2008 to
January
2012. Eligible patients for laparoscopic surgery,
initially were those with benign lesions causing pain or morbidity and
those
suffering from malignant lesions confined to the kidney, with no
evidence of
extension into the renal vein or surrounding tissues.As
experience was gained, more complex procedures were done. In the
present study,
we report all LN performed for 45 months from the first laparoscopic nephrectomy in September 2008. All LN are
posted, those
that were made for benign and malignant pathology.
Surgical
reports were reviewed from a protocol of LN,
which begins its filling in the operating room prior to the start of
the
surgery and is completed at the discharge from the hospital. We
analyzed
demographics, details of the surgery, boarding, surgical technique and
complications. Later, in outpatient clinicsthe
histopathological diagnosis is studied.
Results
In a
period of four years, a total of 200 laparoscopic
kidney surgeries was performed in the HCG by urologists trained in
laparoscopy
(RLA / MGS), or by residents under direct supervision. Of these, 150
were
nephrectomies2, 3 (simple and radical), 15 pyeloplasties
and 35 symptomatic cysts. All nephrectomies
were
developed by transperitoneal approach.
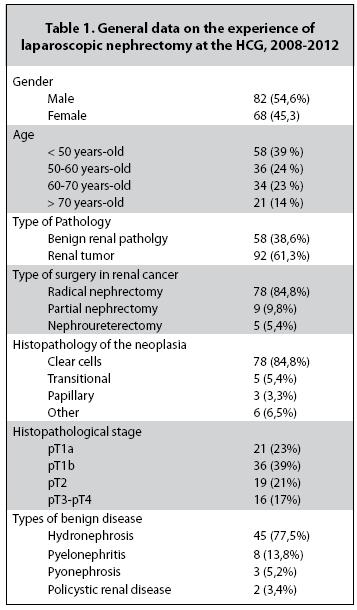
According
to the age groups,cases
were divided in patients under 50 years old, 51 to 60 years old, 61 to
70 years
old and older than 70 years old, corresponding to 39, 24, 23, and 14%,
respectively . The 45% of patients were women and 55% were men. There
were 70
right and 80 left nephrectomies.
Of the 150
LN, 92 were performed because of kidney
cancer and 58 were due to benign pathology. Of the 92 LN due to kidney
tumors:
78 were radical, 9 partial and 5 nephroureterectomies.
According to the pathology reports: 78 were clear cell carcinoma, 2 oncocytomas, 2 chromophobe,
2 angiomyolipomas, 1 papillar
carcinoma, 1 leiomyoma with malignant
potential, 1
chronic pyelonephritis and 5 transitional
cell
tumors.
The
average neoplastic
kidney weight was
A total of
six surgeries had to convert into
conventional open surgery (3%) and 4 to hand-assisted surgery (2%). The
main
reasons for conversion were: 5 laparoscopically
uncontrollable bleeding, 4 because of little progress in surgery and
one due to
ascending colon injury by adhesions. Blood transfusion had to be
performed in 3
patients. 58% of the surgeries were performed with three trocars,
31% with four trocars, 7% with five trocars and 4% with a trocar
for
hand-assisted surgery. The average bleeding per procedure is 164 cc.
Surgical
time used during each surgery is 129 min, on average.
The
removal of the kidney was performed in 62% of
cases, with a Pfannenstiel incision in 17%
of the
cases, infraumbilical midline on 7%, by
the right
iliac fossa, on 7%, by the left iliac fossa, 5%, by expansion of a trocar,
and 2%, through the navel .
Discussion
Open nephrectomy has been
established as the procedure for treating many benign and malignant
renal
diseases. The morbidity of the procedure is due to the incision made in
both transabdominal approach as in
lumbotomy.4, 5 With
laparoscopic surgery this wound can be done in a less morbid area in
order to
remove a diseased kidney and lessen the postoperative pain, analgesic
use,
hospital stay, recovery time and the rate of transfusion;
significantly.
Oncological
outcomes, surgical times, esthetic results and complexity of the cases
are
comparable to global centers of excellence in these procedures.
Nowadays,
with the widespread use of ultrasound and
computed axial tomography (Fig. 3), the diagnosis of benign and
malignant renal
diseases is done on earlier stages and in younger patients.
The
current goal of minimally invasive surgery is to
perform procedures with the same results of traditional surgery, but
with less
morbidity and mortality. This is achieved with increased surgical
skills and overcoming
the initial learning curve.6 Laparoscopic surgery requires a lot of
training
and dedication.
In the
Urology Department of HCG 97% of surgeries due
to kidney tumors and benign renal diseases are performed by a
laparoscopic
approach, which has been of great importance to the Department, because
the
rotation of hospital beds is very high and more patients can be
admitted to
solve a greater number of urological disorders.7 A disadvantage of the
program
is that because almost all procedures are performedby
a laparoscopic approach, residents are less likely to perform open nephrectomies. However, they are acquiring
skills in a
surgical approach that was almost nonexistent in the country five years
ago.
References
1. Clayman R. Laparoscopic nephrectomy. N Engl J Med 1991; 324:1370-1371. [ Links ]
2. Gill
3. Kerb K. Laparoscopic nephrectomy. BMJ 1993; 307:1488-1489. [ Links ]
4. Chatterjee S. Permanent flank bulge is a consequence of flank incisión for radical nephrectomy in one half of patients. Urol Oncol 2004; 22:36-39. [ Links ]
5. Parra R. Comparison between standard flank versus Laparoscopic nephrectomy for benign renal disease. J Urol 1995; 153:11711174. [ Links ]
6. Higashihara E. Learning curve and conversion to open surgery in cases of Laparoscopic adrenalectomy and nephrectomy. J Urol 1998; 159:650-653. [ Links ]
7. Grills R. The Impact of Laparoscopic Nephrectomy on patients outcome: A community Perspective. J End 2011; 25:781-786. [ Links ]


{kind=link}