










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkActa Médica Costarricense
On-line version ISSN 0001-6002Print version ISSN 0001-6012
Acta méd. costarric vol.55 n.1 San José Jan./Mar. 2013
Original
Description
of testicular germ cell tumors, according to biopsies from the
department of
pathology,
Julia Freer-Vargas, 1 Konstantin Liannoy, 2
Authors
affiliations:
Abbreviations:
SD,
standard deviation;TGCT,testicular
germ cell tumor.
Abstract
Background:
95% of testicular tumors are germ cell tumors (TGCT). These neoplasms
have increased in number and have become more common in young people.
The TGCTs are divided into two groups: seminomatous
and non-seminomatous. The objective is to
describe the
TGCT based on pathological biopsy results at the
Methods:
A descriptive study of the department of Pathology database, from which
the
cases of TGCTs were selected. Within the
analysis,
absolute and relative frequencies, confidence intervals, measures of
dispersion
and central tendency were calculated. Chi-square p <0.05 was used
for the
trend.
Results:
148 patients with germ cell tumors were selected. There was an
increasing
tendency in tumors with p <0.003. Out of the total number of cases,
60.2%
(89), CI 95% (52.2-68.1), occurred in males younger than thirty years
old. Non-seminomatous TGCTs
occurred in
59.5% (88) of the cases, CI 95% (51.5-67.3). The average age of those
with non-seminoma was 26.4 years; DE 8.1,
and of those with seminoma was 31 years;
DE 7.5, with a difference of p
<0.001.
Conclusions:
There is a significant tendency towards the increase of TGCT, which is
more
frequent in patients under 30. The non-seminomatous
TGCTs are the most frequent. The average
age for non-seminomatous TGCTs is
significantly lower than for the seminomatous.
Limitations: incidences and prevalence
were not calculated. Recommendations: to focus detection campaigns on
the
population at risk, and extend the study to other hospitals.
Key words:
Germ cells, seminoma, biopsy,
95% of the
tumors arise from germ cells. These tumors
are divided into two groups: seminomatous
and
nonseminomatous (more
aggressive
tumors).2-8 The seminomatous
are characterized by the presence of seminoma
only,
whereas, the nonseminomatous present
embryonic
carcinoma, yolk sac tumor, choriocarcinoma
and/ or
immature or mature teratoma. Furthermore,
TGCT are
characterized by combinations of two or more types of different tumors
mentioned above.3
The risk
factors that are considered in the
development of these tumors are: cryptorchidism,
congenital malformations (hypospadias),
intersexual
syndromes, Caucasians, family history, etc. There arealso
acquired risk factors: prenatal risk factors (high estrogen levels),
child
nutrition, western lifestyles (little exercise, caloric diets),
occupation
(welders, painters, carpenters), 1-5 etc. It is well known
that the
higher incidence occurs in northern European countries such as
Most
authors report that 35.7% of the TGCTs are
seminomatous5 and they are diagnosed
between 30 to 50 years old, with a mean age of 35.8, SD 8.6,5-6
while non seminomatous tumors
present in 64.2%
of cases,5 and these are most common in adolescence and
early
forties, with an average age of 29.1 years, and a SD of 8.9.6-5
This study
was conducted in
The aim of
the study was to characterize the TGCT
based on the results of the biopsies done at the department in the
Methodology
It was a
descriptive study conducted at the
The
inclusion criteria were all results of testicular
biopsies to which the procedurewas
performed in the study
period (from January 1, 2003 to March 31, 2011). Results of no neoplastic and neoplastic
biopsies from the same patient were excluded. All cases of germ cell
tumors
were selected for the study.
For
statistical analysis, we used Epi
info 3.3.2 and Microsoft Excel. The results of the TGCT are presented
using
tables and figures, which show the distribution according to tumor
type, group,
age, and according to the predominance of mixed tumor.
The study
protocol complied with the requirements of
the Institutional Review Boardof the
hospital where
the study was performed.
Results
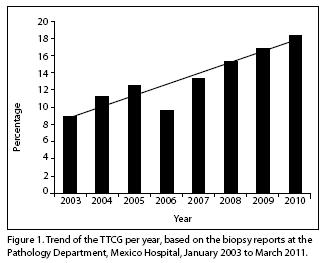
In the
study period, there were 1455 testicular biopsy
results revised of which 148 cases of TGCT were selected, with an
average of
18.1 cases per year, with a DE of 4.1, with a minimum of 14 cases per
year and
a maximum of 22 cases per year. The annual trend of TGCT was measured
using a
Chi square trend, and there was a significant riseof
p <0.003 (Figure 1).
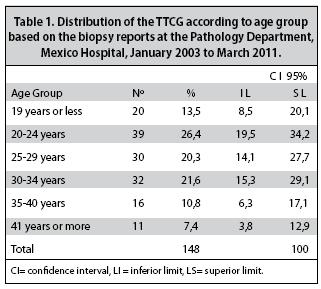
The
average age for the TGCT was 28.3 years, with a SD
of 8.2 and a range for the age of 14-56 years. It was determined that
60.25%
(89 cases, 95% CI 52.2-68.1) had 29 years or less, and 39.8% (59 cases,
95% CI
31.9-47.7) had 30 years or more, and the most affected group was that
of 20 to
24 years where there was the highest percentage of cases (Table 1).
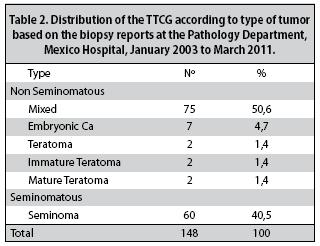
According
to the classification of TGCT, we found that
40.5% (60 cases) 95% (32.6-48.4) were seminomatous
type, and 59.5% (88 cases, 95% CI 51.5-67.3) were non seminomatous
type: the mixed tumor was the most frequent, it presented in a 50.6%
(75 cases)
(Table 2).
The
average age for nonseminomatous
type was 26.4 years, SD 8.1, with an age range of 14 to 56 years, and
for seminomatous type it was 31 years, SD
7.5, range 18 to 54
years. The calculated difference in these averages for age is
significant at p
<0.001.
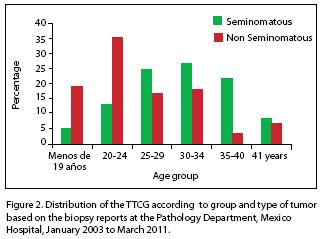
When
comparing both tumors by age group, we found that
the highest percentage of non-seminoma
tumors
occurred in the group of 20 to 24 years, in a 35.2% (95% CI 25.2-45.2),
while
for the seminomatous tumors, it appeared
in the group
aged 30 to 34 years with 26.7% (16 cases, 95% Percentage CI 15.4-37.8)
(Figure
2).
In 71.5%
(63 cases, 95% CI 62.1-81.1) of nonseminomatous
tumors there was an age under 30 years,
while in the case of seminomatous tumors,
it was
43.3% (25 cases, 95% CI 7.30- 55.8).
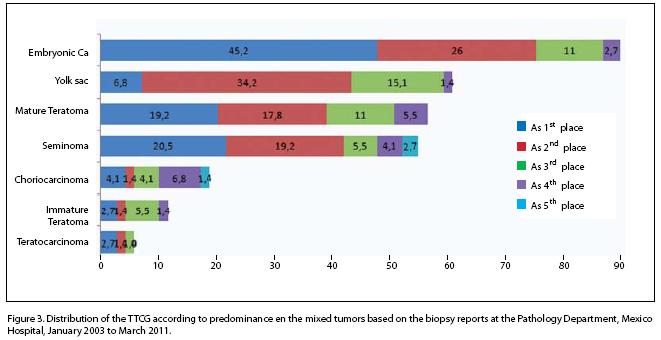
Furthermore,
it was found that 84.9% (64 cases) of
mixed tumors diagnosed were embryonic carcinoma, predominant in 45.2%
(34
cases) (Figure 3).
Discussion
There is a
significant trend towards an increase in
the detection of TGCT compared with other countries. The average age of
TGCT
was lower than that reported in the literature, and it occurs most
often in
children under 30 years, statistically significant.1,3,4
According
to the classification of TGCT type, nonseminomatous
tumors are significantly more frequently in
comparison with the literature data.1
There are
significant differences in the average age
of both tumors, and patients with nonseminomatous
TGCTs were younger (30 years or younger),
including the group
of 20 to 24, whichis the most affected.
When
comparing the average age of seminomatous TGCTs with data from the world literature, it is
significantly lower. In patients with nonseminomatous
TGCTs, the average age is also lower, but
it does not
reach significant differences.
From the nonseminomatous TGCTs,
the mixed tumor is the most common; and embryonic
carcinoma is the dominant tumor manifestation, similar to the
literature data.
A
limitation of this study is that because of the type
of study it is not possible to establish causal relationships. The
study is not
population based, which prevents the calculation of the incidence and
prevalence of disease.
It is
recommended to direct detection campaigns for
youth and young adults, to do association studies, to expand it to
other
national hospitals in order to understand the behavior and also to
analyze the
trend in
Conflict
of interest: There is no conflict of interest
because thisstudy was performed as part of
the daily
work that helps us daily in the decision-making at our hospital.
References
1. American Cáncer Society. Cancer de testículo. Atlanta, Georgia: 23 marzo 2011. [ Links ]
2. Richie J, Steele G. Neoplasias del Testículo. En: Patrick C. Walsh. Campbell Urología, 8 ed. Uruguay: Editorial Médica Panamericana: 2002. 3147-3154. [ Links ]
3. La llave F, Lomas M, Laguna E, Asuar S, Murillo J, Ramírez A, et al. Estudio Descriptivo de los tumores testiculares germinales: 13 años de experiencia en el área de Salud Badajoz. Arch. Esp. Urol. 2007; 60: 531-537. [ Links ]
4. Gorena M, Cinfuentes M, Gonzalez R, Villagran J, Hinostroza Ja, Pastor P, et al. Perfil clínico y epidemiológico del Cáncer Testicular en la Región. Rev Chil de Urol. 2003; 68: 78-82. [ Links ]
5. Gutiérrez–Tejero F. Revisión Histogenéticos de los tumores testiculares Germinales (Tesis doctoral). Granada: Universidad 2007; 93-136 5. [ Links ]
6. Ministerio de Salud de Chile. Guía Clínica Cáncer de testículo en personas de 15 años y más. Santiago Chile: MINSAL 2010. [ Links ]
7. Saavedra J, Ramírez C Peña G, Stoopen M, Barois A, Kimura Y. Cáncer de testículo. An Radiol Mex. 2009; 1:47-59. [ Links ]
8. Gk Jacolsen, H Barbelo, J Olsen. Testicular germ cell tumors in
9. SJ Harland. Intratubular germ cell neoplasia of the contralateral testis in testicular cancer: Defining a high risk group. J Urol 1998; 160: 1353-1357. [ Links ]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}