










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkActa Médica Costarricense
On-line version ISSN 0001-6002Print version ISSN 0001-6012
Acta méd. costarric vol.54 n.4 San José Oct./Dec. 2012
Original
Prevalence
of intestinal parasites in food handlers in a rural community in
Gilberto Bastidas,1 Carolina Rojas,2
Elisa Martínez-Silva,3 Lisbeth Loaiza,4 María
Guzmán,5 Varuna Hernández,5 Luis Rodriguez,5
Flor Rodríguez,5 Lesbia Meertens5
Authors’
affiliations:
Public
Health Department, Public Health and Social
Development School, Health Sciences Faculty, Universidad de Carabobo
(Carabobo
University), Venezuela.1 Dr. Egor
Nucete Hospital. San Carlos, Estado
Cojedes, Venezuela.2
Investigation and Professional Development Department, Bioanalysis School, Health Sciences Faculty,Universidad
de Carabobo, Venezuela.3 Parasitology
Department,Biomedical Sciences School,
Public Health
Faculty, Universidad de Carabobo.4 Public Health
Department, Public
Health and Social Development School, Health Sciences Faculty,
Universidad de
Carabobo, Venezuela.5
Correspondence:
bastidasprotozoo@hotmail.com
Abstract
Aim: Intestinal
parasites are a public health problem due to their high prevalence.
Handlers of
food contaminated with parasites become potential sources of infection
because
some parasitic forms are transmitted directly from the source of
infection to
the host through the fecal-oral route. In addition, there is an
increased
consumption of food outside the household by residents of urban and
rural
areas. The objective is to collect information so that health
authorities
implement health programs appropriate to each region.
Methods: Descriptive
and cross-sectional field-study. Sixty-four food handlers participated
but
the sample
was composed of
Results: The sample
was composed of44 women and 6 men, 52% belonged to the IV stratus; most
knew
about hygienic practices in food handling but 26% had some form of
intestinal
parasites; the most frequent were: E. nanny (41.2 %) and B. hominis
(38.7 %); monoparasitism was 54%.
Conclusion:
Several
factors are involved in the occurrence and frequency of intestinal
parasitic
disease. Therefore, educating food handlers about good hygiene
practices
according to the environment is essential to prevent transmission.
Key Words:
Intestinal parasite, food handler, habits, feces, prevalence.
Intestinal
parasites are a public health issue, nearly
2000 million people are at risk around the world, 300 million have
associated
morbidity and 155000 die annually.1-5 The etiologic agents
include: Ascaris lumbricoides, Trichuris
trichura, Ancylostoma
duodenal Entamoeba histolytica
and Giardia
intestinalis, the global prevalence of ascariasis is estimated in 1450 million, 1050
million for trichuriosis and 1300 million
are infected with hookworm,
amoebas cause 450 million infestations and about 100,000 deaths per
year; and
finally, giardiasis is considered the most
common
parasite disease in children, responsible for no less than 4000
hospital
admissions each year.6
Even
though in Venezuela a health certificate is
mandatory for food handlers, this is annually renewed, therefore,
health
control is late, enhancing the role of enteroparasite
spread by food handlers, with special emphasis on those preparing food,
considered high risk not for the possibility of becoming ill, but
because their
work implies a higher responsability.13 It should also be
taken into
account, the increase in food consumption outside of the family core,
initially
for urban areas, but now also for rural areas because of transculturation,
where itinerant food stands now appear and persist over time.13-15
Thus the
aim of this work was to investigate the epidemiology
(gender and socioeconomic conditions) and hygiene practices to prevent enteroparasitic diseases in food handlers, at
the rural
community of Manrique, Cojedes State,
Venezuela, a
region like others in the country, with economic delay and
underdevelopment,
where never made such studies in order to provide information on such
diseases
to health authorities, to implement health programs appropriate to the
reality
of life in each region.
Method
Population
and Sample: This
was a descriptive, field and transverse study. The research was
conducted at
the Manuel Manrique parish, located at
480m altitude,
upstate
Hygienic
practices and socioeconomic status: In
accordance with the study´s objectives, a
research questionnaire was applied, commonly used in other areas of the
world,
but validated by specialists in the field, to be applied in the study
area, to
measure preparation, service and kitchenware cleaning hygiene
practices,
followed by the Manrique community
subjects in terms
of food handling.
In each
questionnaire a maximum score of five (5)
points and a minimum of one (1) was
established for
each item. To determine these scores, each subject was given three
response
options: never (1 point), sometimes (2 points) and always (3 points),
in five
of seven questions, based on which the proposal was evaluated, for this
purposes, each option was signaled with an “x”; there was only one
dichotomous question and another one showed two possibilities. The Graffar method, modified by Méndez-Castellano
was applied to determine the family´s
socioeconomic status on the sample, which allowed grouping into five
socioeconomic strata: I (high quality of life), II (moderate quality of
life),
III (low quality of life), IV (relative poverty) and V (extreme
poverty).16
Similarly, identification and filiation data were recorded.
Processing
and analysis of stool samples: The
samples were analyzed by specialized personnel, using the direct stool
examination, which uses isotonic saline (0.85% NaCl).
Also, the modified direct method was used, which is based on Lugol´s iodine solution (
The
resulting preparations were coated with 22x22mm
cover glasses and analyzed microscopically with 10x
and 40x zooms. As a complementary aspect of this research and to
identify helminth eggs; Kato Katz, Willis
and Faust concentration
methods were applied.17, 18 All
individuals
with intestinal parasites were treated with specific anti-parasitic
drugs.
Serial parasitological examinations was the preferred method to
determine
intestinal parasitosis.19
Statistical
analysis: Data
obtained from both questionnaires: measures for food handling practices
and
measures to assess socioeconomic status, as well as, gender-related
data and coproparasitologic test results,
were introduced in a
database created with the Epi Info
5.0statistical
program.20 The obtained
information was
analyzed through descriptive statistic methods.
Results
The sample
consisted of 50 apparently healthy food
handlers, between ages 20-40, 44 women (88%) and 6 men (12%). Of these
individuals, 52% belonged to stratum IV (relative poverty), 34% to
stratum III
(low quality of life), 10% to II (moderate quality of life) and 4%
belonged to
socioeconomic stratum V (extreme poverty ), none qualified for stratum
I
(quality of life), according to the Graffar socioeconomic stratification scale,
modified by Méndez Castellano.22
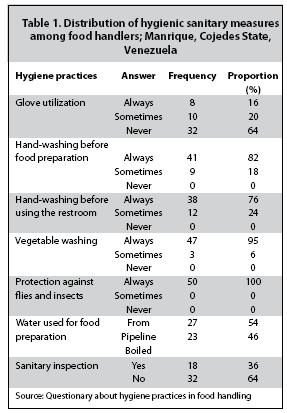
Regarding
hygiene practices followed by the subjects, over
75% of individuals referred washing their hands after using the
restroom and
before preparing food, but 64% do not use gloves to serve it. Also,
between
95-100% of them wash vegetables before preparing them and protect food
from
arthropods. However, only 46% use boiled water and receives sanitary
surveillance (Table 1).
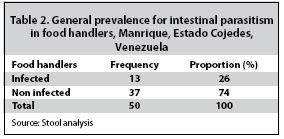
Stool
analysis showed 13 individuals (26%) with some
intestinal parasitosis, including all men,
but 37
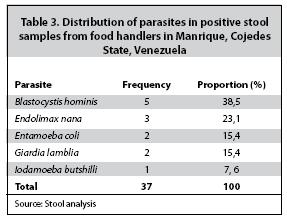
(74%) did not show intestinal parasites (Table 2). The
parasite species, all protozoan, most
frequently observed in positive samples
were: Blastocystis hominis
(38.5%), Endolimax nana (23.1%),
Entamoeba coli (15.4%), G.
intestinalis (15.4%) and Iodamoeba
butshilli (7.6%) (Table 3).
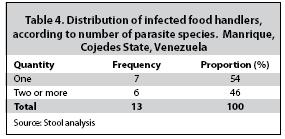
As for the number of infecting species, 54% were parasitized by single
species
and the rest (46%) had two or more parasites (Table 4). The
predominant
parasite association was between B. hominis
and E.
nana (27%).
Discussion
The female
over male prevalence could be because the
number of male representatives in the sample was affected by work
reasons,
because men are mainly involved in agricultural activities in the area,
or
other tasks that require moving to urban regions in the
Also, food
handling hygiene measures can be considered
relatively satisfactory, although a proportion of the sample,
regardless of
their socioeconomic class, had parasites transmitted through the
fecal-oral
route, which shows the ease of transmission from person to person,
despite
State health controls.13 Possibly, the
knowledge they
have about proper food handling is the product of information
transmitted by
communication media.22-24
Oral-fecal
transmission of parasitosis
in food handlers registered in this study (26%), is similar to that
reported in
populations from Brazil (17%) and Colombia (17%), and the prevalence of
protozoa, a phenomenon that is probably a result of inadequate
sanitation and
water supply.13,25 B. hominis
(38.5%)
was the parasite with the highest incidence, above the national average
(around
10%), followed by E. nana (23.1%), protozoa with a doubtful pathogenicity, but considered markers of
fecal-oral
contamination, and which together constitute the predominant parasitic
association in this writing (27%). Similar studies in other Latin
American
countries show, for example, that polyparasitism
(46%
of cases) reported in this investigation is twice higher than that
found in
Nicaragua; and regarding the most frequent parasite infecting people,
described
findings are similar to those reported in Chile, where E. nana,
with
46.6%, was the most found, followed by E. coli (41.2%) and E.
histolytica (12.1%)13,15,25-29
Towards
the inner side of
It has
been told that the solution is not to eradicate
street food vendors, but getting people to understand the essentials of
hygiene
in food preparation, within formal health programs, consistently
applied, with
continuous monitoring, focused and adhered to the local and cultural
aspects
that define each population.32-34
Conflicts
Of Interest: It is cleared that there are no
commercial associations that may mean a conflict of interest with this
article,
and that this research was fully funded by the authors.
References
1. Anderson R, May R. Population dynamics of human helminthic infections: Control by chemotherapy. Nature 1982; 287:557-63. [ Links ]
2. Cooper E. Intestinal parasitosis and the modern description of diseases of poverty. Trans R Soc Trop Med Hyg 1991; 85:168-70. [ Links ]
3. Lynch N. Influence of socio-economic level on helminthic infection and allergic reactivity in tropical countries. En: Moqbel R, editor. Allergy and immunity to helminths: Common mechanisms or divergent pathways? London: Taylor and Francis; 1992; 51-62. [ Links ]
4. UNICEF (1999). El estado de salud infantil: una emergencia silenciosa. New York; 1999. [ Links ]
5. OMS. Alerta sobre infección de parásitos intestinales en países en desarrollo. 2008. En: http://www.un.org/spanish. consultado el 24 de junio de 2011. [ Links ]
6. Woo P, Paterson W. Giardia lamblia in children in day care centers
7. OPS-OMS. Atención integrada a las enfermedades prevalentes de la infancia. AIEPI. Reunión sobre el control de las helmintiasis intestinales en el contexto de AIEPI, 1998; 184. [ Links ]
8. OPS/OMS. Helmintiasis intestinal. Manejo de la helmintiasis. Departamento de Parasitología y Microbiología de la Universidad de la República de Uruguay, 2003. [ Links ]
9. WHO. Schistosomiasis and soil-transmitted helminthiasis—an unprecedented opportunity for control. In: WHO. Communicable Diseases 2002 - Global defence against the infectious diseases threat. World Health Organization, Geneva, Switzerland, 2003. [ Links ]
10. Devera R, Niebla P, Nastasi C, Velásquez A, González M. Prevalencia de Trichuris trichiura y otros enteroparásitos en siete escuelas del área urbana de Ciudad Bolívar, Estado Bolívar, Venezuela: Saber 2000; 12: 41-7. [ Links ]
11. Hagel I, Salgado A, Rodríguez O, Ortiz D, Hurtadp M, Puccio F, et al. Factores que influyen en la prevalencia e intensidad de las parasitosis. Gac Med Caracas 2001; 1:82-90. [ Links ]
12. Gubia L, Galanternink L, Galan G, Cabrera J, Durango M. Staphylococcus aureus: Sensibilidad antibiótica y detección de enterotoxinas de cepas aisladas de alimentos y manos de manipuladores. Rev De Cien 2004; 30:12-4. [ Links ]
13. Lozano S. Parasitosis de transmisión directa en personal manipulador de alimentos bajo un programa de salud ocupacional en el Distrito de Santa Marta durante el año 2006. Salus 2009; 6:112-7. [ Links ]
14. Forsythe S, Hayes P. Higiene de los alimentos. Microbiología y HACPP. Segunda edición. España: Editorial Acribia, 2002. [ Links ]
15. Mollinedo P, Prieto B. El enteroparasitismo en Bolivia (Memoria de la investigación 1975-2004). Elite impresiones.
16. Méndez-Castellano H, Méndez M. Sociedad y estratificación. Método Graffar-Mendez Castellano. FUNDACREDESA. Pag. 0206. p. serie. 0. Abierta. [ Links ]
17. Botero D, Restrepo M. Parasitosis humanas. Corporación para investigaciones biológicas 3 era Edición. Medellín Colombia 1998; 457pp. [ Links ]
18. Faust E, D’antoni J, Odon V, Miller J, Perez C, Sawitz W, et al. A Critical study of clinical laboratory techniques for the diagnosis of protozoan cysts and helminth eggs in feces: preliminary communication. Ameri J Trop Med 1938; 18:169-83. [ Links ]
19. Piédrola-Angulo G. Diagnóstico de las infecciones. En: Pumarola A, editores. Microbiología y Parasitología Médica. Editorial Salvat,
20. Dean, A, Dean J,
21. Méndez-Castellanos H, López B, Landaeta J, Gonzales T. Estudio transversal de Caracas. Arch Venez Puer Ped 1986; 49:111-55. [ Links ]
22. Cortés D, Estrada M, Areas K, Téllez A. Frecuencia de parásitos intestinales en expendedores de alimentos ubicados en los recintos de
23. Cirocco P, Bolivar A, Vilé J, Cirocco A. Leishmaniasis: evaluación de los conocimientos en poblaciones pertenecientes al Distrito Sanitario Nº 3 del Estado Miranda, Venezuela. 2000. En: http://www.svm.org.ve/documentos/volumen. Consultado el 30 de junio de 2011. [ Links ]
24. Alleyne G. La equidad y el futuro por labrar en el campo de la salud. Rev Panam Salud 2001; 10:371-5. [ Links ]
25. Poma J. Diarreas infantiles relacionadas con la presencia de parásitos (tesis).
26. Castrillo A, González M, Tirado E. Frecuencia de infección por Blastocystis hominis: un año de estudio. GEN. Revista de
27. Devera R, Niebla-Punos G, Nastasi J, Velásquez V, González-Meneses R. Prevalencia de infección por Blastocystis hominis en niños del Estado Bolívar: valor del examen directo de heces en el diagnóstico. In: XV Jornadas Científicas, Tecnológicas y Educativas de Guayana, Memorias, pp. 28-29, Ciudad Bolívar: Asociación para el Avance de
28. Salvatella R, Eirale C, Ballesté R. Endolimax nana (Wenyon & O Connor, 1917) (Amoebida, Endamoebidae) su presencia en la casuística del Hospital de Clínicas, consideraciones sobre su papel patógeno. Rev Urug Patol Clín 2001; 34:35-44. [ Links ]
29. Cortés S, Estrada L, Areas B, Téllez S. Frecuencia de parásitos intestinales en expendedores de alimentos ubicados en los recintos de
30. Freites A, Colmenares D, Pérez M, García M, Díaz O. Infección por Cryptosporidium sp y otros parásitos intestinales en manipuladores de alimentos del Estado Zulia, Venezuela. Invest Clin 2009; 50:13-21. [ Links ]
31. Requena I, Hernández Y, Ramsay M, Salazar C, Devera R. Prevalencia de Blastocystis hominis en vendedores ambulantes de comida del municipio Caroní, Estado Bolívar, Venezuela. Cad Saúde Pública 2003; 19:1721-7. [ Links ]
32. Catruista T, Monroy T. Enfermedades infecciosas y nutrición. Ide@s CONCYTEG 2009; 4:779-86. [ Links ]
33. Gustavsen K, Hopkins A, Sauerbrey M. Onchocerciasis in the
34. Incani RN, Hernández M, González ME. Hyperinfection by Strongyloides stercoralis probably associated with Rituximab in a patient with mantle cell lymphoma and hyper eosinophilia. Rev Inst Med Trop Sao Paulo 2010; 52:221-4. [ Links ]
35. Ferrer E, Sánchez J, Milano A, Álvarez S,


{kind=link}
{kind=link}
{kind=link}
{kind=link}