










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkActa Médica Costarricense
On-line version ISSN 0001-6002Print version ISSN 0001-6012
Acta méd. costarric vol.54 n.4 San José Oct./Dec. 2012
Original
Hyperparathyroid
pathology treated in three Costa Rican hospitals
Manuel F. Jiménez-Navarrete
México,
San Juan de Dios and “Dr. R.A. Calderón Guardia” Hospitals,
CCSS.
Author’s
affiliation: Service of Endocrinology.
San Vicente de Paúl Hospital, Heredia.
Abbreviations: CCSS, Caja Costarricense
de Seguro Social; USA, United States of
America; HCG,“Dr.Rafael Ángel
Calderón Guardia” Hospital;FHH,Familial
Hypocalciuric Hypercalcaemia;
HM, México Hospital; HPT, hyperparathyroidism; HPTp,
Primary Hyperparathyroidism; HSJD,San Juan
de Dios
Hospital; CKD, Chronic Kidney Disease; MEN-1, Multiple Endocrine Neoplasia Type 1; PAHO, Pan American Health
Organization;
PTH, parathormone; PTHi,
intact parathormone.
Abstract
Aim: To
determine the frequency and characteristics of patients who received
treatment
for hyperparathyroid pathologies in the
Methods: Analysis
of records of high serum intact parathormone,
medical
records and bibliographical review. Descriptive study, whose sample was
patients treated between January 2007 and December 2009.
Determination of frequencies and proportions for the qualitative
variables was
made by means of the Chi-Square test. The quantitative variables were
determined by the estimate of Student’s t-test.
Results: Out of 199
patients studied, 9 were excluded. Women prevailed (68.9 %), the most
frequent
age group was 60 years and over (33.1 %). Primary hyperparathyroidism
was the
most frequent disease (n=46, 24.2 %; 73.9 % women, 69.5% older than
50), then hypovitaminosis D and chronic
renal failure. The majority
lived in
Discussion:
Patients
with raised PTH by diverse reasons are exposed to many diseases that
can
compromise their survival and quality of life. Hypovitaminosis
D would probably be more frequent if measurement was requested more
often. The
request for calciphediol must be
emphasized in any
parathyroid disease.
Keywords:
Hyperparathyroidism, PTH, parathormone,
vitamin D.
Hypercalcaemia
is defined as the abnormally high concentration of calcium in the
bloodstream.
There are three known causal mechanisms: increased in bone resorption,
increased gastrointestinal absorption and decreased renal excretion.1,2 The main defense of the organism
against hypercalcaemia is decreasing the
secretion of PTH. This,
will decrease the bone resorption and the
kidney
production of the active metabolite of vitamin D (VD), with the
consequent
decrease of intestinal absorption and increase urinary loss of calcium.2
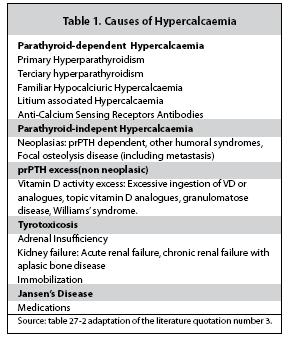
To
address schematically hypercalcaemic
disorders, a
practical way is to establish the dependency and independency to PTH (table 1).3
PTH and VD
are the main regulatory hormones of calcium
homeostasis, and both influence in each other synthesis. The first
stimulate
the kidney enzyme 1αhydroxylase, and the
second has a negative feedback over PTH.4
PTH is a
lineal peptide of 84 amino acids, produced in
the parathyroid gland. Is the regulatory hormone of calcium, phosphate
and VD
concentrations in serum and its classical biologic activities are
mediated by
PTH1R receptors in different tissues. The amino terminal region of the
molecule
possessed the sequence needed to activate this receptor. The metabolism
is
complex: it starts in the parathyroid secretory
granules and ends in diverse tissues, primarily the liver and kidneys;
a series
of “PTH peptides” are presented in serum, in normal conditions and
in diverse states if hyperparathyroidism.5
The
current availability of second generation
bioassays allows a negative feedback, produced by the ionized calcium (
The
activity and the control of PTH is regulated
through an intricate system, in which serum ionized calcium (main
parathyroid
calcium regulator), phosphor, calcitriol
and
derivatives participate with other less studied factors, acting on the
parathyroid gland and influencing in its synthesis and secretion (aluminium, estrogen, magnesium, corticosteroids,
cytokines
and fibroblastic growth factor).23 Several receptors, such
as the
calcium, the vitamin D and the fibroblastic growth factor receptors,
mediate
this system. There are other indirect actions on calcium and vitamin D
receptors, with correlation dependence between calcium, calcitriol
and phosphor. The serum ionized calcium in the parathyroid gland
produces sigmoidal responses in PTH
secretion: small calcium changes
provoke great variations in PTH. An example can be seen when analyzing
the
independent variables.3 It is
considered
that in vivo, PTH different regulatory factors possessed interrelations
that
difficult the interpretation of each role separately.9
Normal
levels of PTH and calcium in serum, does not
necessarily means healthy parathyroid glands, in autopsy reports large
parathyroid glands in patients were found without the presence of
hyperparathyroidism.10 There are also reports of
parathyroid
carcinomas with normal serum levels of calcium. This cancer is an
uncommon
cause of hyperparathyroidism, and presents more frequently in severe hypercalcaemia and high levels of PTHi.11
Elevated
serum PTH with normal calcaemia
is an independent predictor of long term survival prognosis in certain
population groups. Calcium and vitamin D (is the main cause of PTH
elevation),
are not significant long term survival prognosis indicators, especially
in the
elderly.12
Hyperparathyroidism
is the increase secretion of PTH
with or without clinical manifestations. The following are causes of
elevated
PTH, that can be related to different levels of calcaemia:
primary hyperparathyroidism (most common), hypovitaminosis
D, hypomagnesemia, milk-alkali syndrome, granulomatose diseases or neoplasias,
prolonged immobilization, hyperthryroidsm,
adrenal
insufficiency, familial hypocalciuric hypercalcaemia, kidney disease (with creatinine
clearance below 50cc/min), liver disease, hypercalciuria,
malabsorption syndromes, medications (litium, anticonvulsivants,
loop
diuretics, esteroids, biphosphonates),
Paget’s disease and other bone pathologies.13
This
research provides a novelty to
Materials
and Methodology
This is a
descriptive study. The blood samples were
taken from patients with age ≥18 years old, attended in
The record
of different hyperparathyroidism in
The
classification above is used to record only
hospitalized patients, thus it was necessary to appeal to another
strategy with
the purpose of finding the samples collected from outpatients. From the
database
of Hormone and Clinical laboratories of
From all
variables, a distribution according to
absolute and relative frequencies was made. A stratified analysis
according to
genre, age groups, and pathologies associated with hyperparathyroidism,
home
residence and hospital assistance was made. All analysis were developed
through
Epiinfo 3.4.1 (CDC-2007) statistical
software, and
was defined as statistically significant, a critical point of 0.05 (α≤0.05).
This
research was approved by the Medical Directors of
the three hospitals, after the analysis the local committees of
bioethics and research
(CLOBI), endorsed from an ethical and methodological point of view,
recommended
to go through this research.
Results
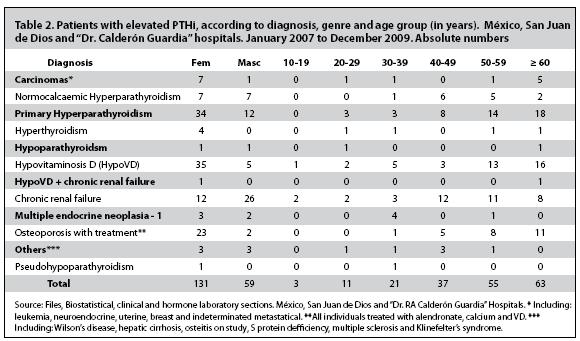
A total of
199 patients were analyzed, in which 9 were
excluded (they were incomplete). From 190 cases, most of them were
females
(68.9%), and the most common age group found were of ≥60 years old
(33.1%), followed by the age group between 50 and 59 years old (28.9%; table
2).
Of the
pathologies found with high PTHi,
the primary hyperparathyroidism was the most common (24.2%; 73.9%
women; 69.5% ≥50
years old), followed by hypovitaminosis D
(21.6%;
87.5% women; 72.5% ≥50 years old), chronic kidney disease (20.5%; 66.6%
men; 30.7% between ages 40 to 49 years old) and osteoporosis with
treatment
with alendronate (13.1%; 92% women; 76%
≥50
years old; table 2).
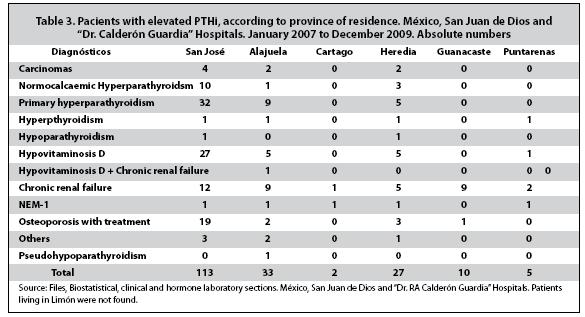
In
relation to the place of residence, the majority
lives in the
In
relation to vitamin D measurement, physicians
don’t give enough relevance to asked for the test in different
pathologies in which are required. For example of the above, the
following
situations have been found: a VD measurement in the majority of hyperparathyroid patients was not requested;
some cases in
where normocalcaemic hyperparathyroidism
was
diagnosed (essential aspect for diagnosis) the measure of VD was not
found. The
request of calcifediol were found only in
14 patients
with primary hyperparathyroidism, with an average of 70.2nmol/L (limit
34.5 to
139nmol/L), in which nine (71.4%) were within limits of insufficiency
and 2.17%
were within limits of deficiency. Three patients diagnosed with PTH,
didn’t have a VD measurement.
Discussion
Individuals
with elevated PTHi,
as a consequences of diverse pathologies representing primary or
secondary hyperparathyroidisms, are
exposed to an elevated risk of
cardiovascular morbidity and mortality, and are an example of many
pathologies
that compromises the patient’s survival and quality of life.15-17
The
majority of studies found in the international medical
library about carriers of diverse pathologies related to elevated PTHi, there are works dedicated to each entity
separately
and the reports of women and elderly were the most common variables.
There were
no reports on the frequency of different hyperparathyroid
pathologies analyzed jointly. Multiple references about the incidence
and
prevalence of each pathology are mentioned,
but a
comparative study between findings cannot be done.
The most
common entity found in this study is primary
hyperparathyroidism, followed by hypovitaminosis
D,
although this last one could have been more frequent if its measurement
was
done more frequently.
This
research found that the most common pathologies
(primary hyperparathyroidism, hypovitaminosis
D and
osteoporosis) are higher in frequency in women and elderly, while
chronic
kidney disease was more frequent in men and younger individuals.
The record
of diverse problems related to the
parathyroid glands is scarce in the studied hospitals. Many physicians
don’t follow the requirements needed to approach these pathologies.
It draws
attention, when discussing with physicians
and analyzing the clinical files, that occasionally the concept is not
clear,
and the diagnosis of these pathologies are disdain (for examples normocalcaemic hyperparathyroidism).
The
measurement of calcifediol
in
Study
Limitations
The
majority of individuals with hyperparathyroidsm
are overruled in these three hospital’s outpatient departments. There
is
not enough information in the medical record offices, to structure a
more
complete research.
Another
limitation parts from the difficulty to search
for hyperparathyroid patients in the CCSS,
associated
with problems with its classification and the fact that medical record
offices
take into account hospitalized patients and not the ones in the
outpatient
departments. The CIE-10 section for hyperparathyroid
pathologies
is ambiguous; diverse cases of secondary hyperparathyroidism could be
classify
in item E21.5, and because the workers of Medical record offices are
not
medical professionals, they don’t have clear and aren’t indicate
where to write down the diagnosis. Thus, the analysis of the provided
lists was
made from the hormone laboratory from the hospitals mentioned above.
In San
Juan de Dios hospital laboratory, the only way
to analyzed the PTHi records were to print
them all,
implying a huge expense of stationery, which the hospital management
wouldn’t authorized. Also, of the departments that treat hyperparathyroid patients, only the
Endocrinology
department possessed a database of the movements of patients in the
outpatient
department. The above influence in
the compiled
samples, for it is expected, that the cases of hyperparathyroidism were
much
more than registered. The patients found in this hospital were only
those found
in the clinical files of the outpatient departments of Endocrinology
for a three
year period.
“Dr.
Rafael Ángel
Calderón Guardia” hospital’s
hormone laboratory doesn’t possess a database of different hormones
reports. A few months earlier to this research, the measure of PTHi in this hospital was only starting, thus, a
printed
list of this hormone measurement could be obtained.
San Juan
de Dios and “Dr. Rafael Ángel Calderón
Guardia” hospitals should have a database similar to the one in
The
samples were compiled from the outpatient
departments of endocrinology, internal medicine, urology and metabolic
diseases
of these three hospitals. Enough representation of patients with this
diagnosis
was not made, and is not a reflection on the incidence or prevalence of
this
pathology in a national level.
The
compilation time period of samples was short, with
hardships in the capture of more patients, due to the underrecords
of the biostatistical and files offices,
file
location and clearing up of the diagnosis by some physicians.
The
relevance of this work in
Conflict
of interest: The
author declares no conflict of interest.
References
1. Dox IG, Melloni BJ, Eisner GM y Melloni JN. Diccionario Médico Ilustrado Harper Collins. Editorial Marbán.
2.
3. Kronenberg HM, Melmed S,
4. Guyton & Hall. Fisiología Médica. XI edición. Capítulo 79. Página 978. Elservier España, S.A. Madrid, España 2006. [ Links ]
5. Vieira JG, Kunii I, Nishida S. Evolution of PTH Assays. Arq Bras Endocrinol Metab 2006; 50: 621-627. [ Links ]
6. Boudou P, Ibrahim F, Cormier C, Chabas A, Sarfati E and Souberbielle JC. Third- or Second-Generation Parathyroid Hormone Assays: A Remaining Debate in the Diagnosis of Primary Hyperparathyroidism. J Clin Endocrinol Metab 2005; 90: 6370-6372. [ Links ]
7. D’Souza-Li L. The calcium-sensing receptor and related diseases. Arquivos Brasileiros de Endocrinologia e Metabologia 2006; 50: 628-39. [ Links ]
8. Talmage RV, Lester GE and Hirsch PF. Parathyroid hormone and plasma calcium control: an editorial. J Musculoskel Neuron Interact 2000; 1:121-126. [ Links ]
9. Carrillo-López N, Fernández-Martín JL, Cannata-Andía JB. Papel de calcio, calcitriol y sus receptores en la regulación de la paratiroides. Nefrología 2009; 29:103-108. [ Links ]
10. Akerstrom G, Rudberg C, Grimelius L, et al. Histologic parathyroid abnormalities in an autopsy series. Hum Pathol 1986; 17:520-7. [ Links ]
11. Messerer CL, Bugis SP, Baliski C and Wiseman SM. Normocalcemic parathyroid carcinoma: an unusual clinical presentation. World Journal of Surgical Oncology 2006; 4:10. [ Links ]
12. Björkman MP, Sorva AJ and Tilvis RS. Elevated serum parathyroid hormone predicts impaired survival prognosis in a general aged population. Eur J Endocrinol 2008; 158: 749-53. [ Links ]
13. Lavin N. Manual of Endocrinology and Metabolism. IV edition. Chapter 25, Section V, page 338. Wolters Kluwer with Lippincott, Williams & Wilkins. Baltimore, USA, 2009. [ Links ]
14. Organización Panamericana de
15. Andersson P, Rydberg E, Willenheimer R. Primary hyperparathyroidism and heart disease: a review. Eur Heart J 2004; 25:1776-1787. [ Links ]
16. Garcia de
17. Block GA, Klassen PS, Lazarus JM, Ofsthun N, Lowrie EG, Chertow GM. Mineral metabolism, mortality, and morbidity in maintenance hemodialysis. J Am Soc Nephrol. 2004; 15: 2208-2218. [ Links ]


{kind=link}
{kind=link}
{kind=link}
{kind=link}