










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkActa Médica Costarricense
On-line version ISSN 0001-6002Print version ISSN 0001-6012
Acta méd. costarric vol.54 n.3 San José Jul./Sep. 2012
Original
Achievement of Patient Care Standards established by
the Agreement on Management for Diabetic Patients in the
Raj Chapagain K
Alajuelita
Health Area, CCSS.
Abbreviations: AHA,Alajuelita
Health Area; CRSS, Costa Rican Social Security; CG, management
commitment; DM,
diabetes mellitus; MR, medical records; HbA1c, glycosylated
hemoglobin.
Correspondence:
Abstract
Aim: This study
evaluates the level of compliance with quality of care standards for
patients
with diabetes who attend the
Materials
and methods: This
is an analytical observational cross-sectional study based on the data
in the
medical records of the diabetic patients. Consecutive sampling was used
to
analyze the medical records of 500 diabetic patients of the
Forty
health workers from the Area, directly related
to the fulfillment of the rules of Management
Commitment,
were interviewed.
Results: The study
identified that blood sugar level was not indicated to a total of 14
patients
(2.8%).
From the total of patients studied, 197(39.4%) had a blood glucose
level
between 101- 150mg/dl; only 50 patients (10%) had a blood glucose level
<
Conclusion:
Only 25%
of diabetic patients assessed as adequate the attention received at the
Alajuelita Health Area, according to the
parameters of the
management commitment.
Key words:
Management
commitment, Diabetes Mellitus, quality standards, quality of care,
HbA1c,
fasting glucose level.
The Costa
Rican Social Security (CRSS) operates under
the principles of solidarity and universal coverage in the country,
without
discrimination, regardless of origin, race or nationality. However,
internal
factors, such as failure in the fund raising system, increased spending
and
structural problems, have created a tendency to under-funding and
non-sustainability of the institution, since the early nineties.1,2
Because of
this, the international agencies began to
question the investment projects of the CRSS, therefore, it was
determined to
establish a process of modernization in terms of the structure and
institutional functions and resource allocation based on efficiency,
which
stimulate user satisfaction and improve the quality of care.1,2
As a
regulatory tool, “management
commitment” (MC) was created, which sets the standards, rules,
incentives, penalties and assessments and adjustments in the
implementation
period, according to the planning and management control to detect
deviations
in meeting the goals and targets, and the redirection of resources,
seeking to
fit the needs of a given population. From underfunding, international
financial
organizations have recommended the public sector to work more
efficiently and
effectively in organizational management.
In the
early nineties, the state begins to speak of
social sector reform, and within this, the health sector, with a new
direction:
strengthening primary care. In turn, the Ministry of Health becomes a
nationwide health vigilante governing body. The CRSS assumes the role
of
primary care, the preventative part; three levels of health care are
established, according to the level of complexity; the reference and
counter
reference system between levels are promoted, to reduce service
duplications
and the vision of reducing the high hospital cost, by continuing the
specialty
services at various levels, is reinforced.3
A new
institutional expense control mechanism is
implemented, by introducing the new MC instrument, which marks the
quality of
service standards to users by age group, type of disease, and by the
group
according to the clinical characteristics– what becomes a model of
health
spending control-, and the CCSS quality of care (information obtained
from Cerdas Angulo,
Manuel, “Effects
caused by management commitment assessment in the first six months, in
the
Monsignor Sanabria Hospital”,
Puntarenas;
MBA thesis on Sustainable Health Administration, SEP, UNED, Costa Rica,
1997).
One way to
determine compliance with the quality of
care at the primary level, is to study
directly the
compliance of the quality of care in an age group or a group of the
same
disease. In this case a cross-sectional study of diabetic patients in a
health
area was developed, as their high national prevalence and the high cost
of care
is an important issue.
This work
aimed to study the compliance of the quality
of care for diabetic users of the Alajuelita
Health
Area (AHA), and the determining factors in the failure to propose
suggestions
to improve it. It tried to show how the physical structure, the lack of
training and health staff equipment contribute to flout the rules
established
in the MC, for the care of diabetic patients in the Alajuelita
Health Area, from January to July 2007.
Materials
and methods
A
cross-sectional observational analytic descriptive
study was conducted, based on data from the records of diabetic
patients of the
AHA,4 in the Alajuelita
community, located south of
The
universe of analysis is the population of
diabetics who have their medical checkups in the AHA. The target
population
consisted of diabetic patients with medical records in the AHA, a total
of:
3088. Using a consecutive sample of the Area, 500 diabetic patient
clinical files
were analyzed to examine level compliance of the quality of their care,
between
January and July 2007. The sample included diabetic patients with
associated
diagnosis of hypertension and ischemic heart disease. Data collection
was
performed using a precoded sheet design
based on that
used for the control of diabetic patients, as part of MC nationwide.
To
complement this, 40 Health Area workers directly
related to the compliance of MC standards were interviewed. 40
employees were
distributed (technicians, doctors, nurses and primary care
technicians), the
questionnaire about the physical plant, ventilation and lighting, space
and
distribution services in the Alajuelita
Health Area.
The
variables that were included on diabetic patient
were age, sex, co morbidities, BMI, fasting glucose control, HbA1c,
cholesterol
and triglyceride levels, diabetic foot, -which was evaluated with
PATONA- and
education. Information was collected from medical consultations during
the
period of January to July 2007.
Results
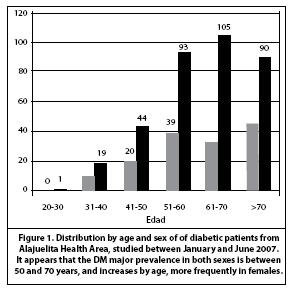
The sample
distribution of the diabetics evaluated by
age and sex are shown in Figure 1. 29,6% of diabetics
are men and 79,4% women. Diabetic women are most prevalent in the age
group between
61-70 years old (21%), while in men prevails the group of >70 years
old,
which is 9,2%.
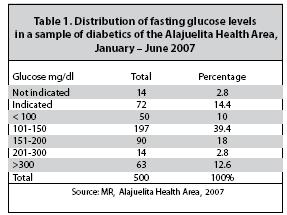
Regarding
the behavior of the blood sugar levels in
diabetics in the AHA, it was revealed that 2,8% of the sample were not
given
the test; 14,4% were given, but the result was not found in the file;
39,4% had
blood glucose level between 101-150mg/dl; only 50 patients had blood
glucose
< de 100, which is 10%. In addition, 14 patients (2,8%)
had a fasting blood glucose level between 201-300 mg/dl. Of these 500
patients,
63 had a fasting blood glucose >300, which is 12,6%
of people poorly controlled (Table 1).
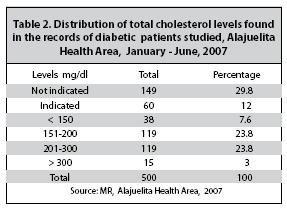
The
distribution of total cholesterol levels in
diabetics that were studied shows that 29,8%
of
patients were not at all given the test (Table 2). 47,6%
of theses diabetics maintain the level of total cholesterol between
151-300mg/dl. Only 123 patients maintain a cholesterol <150 mg/dl,
which is
24,6%. The study found that 60 diabetics
(12%) did not
have the total triglyceride levels indicated.
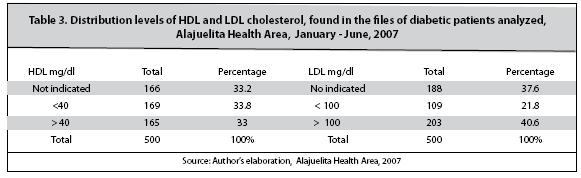
166
patients were not at all given the HDL cholesterol
test, which is 33,2%. Similarly, 188 were
not noted in
the study of the LDL levels (37,6%). Only
165 diabetic
patients (33%) have an adequate level of HDL, which is > 40 mg/dl;
169
maintain the level of HDL cholesterol <40 mg/ dl (Table 3).
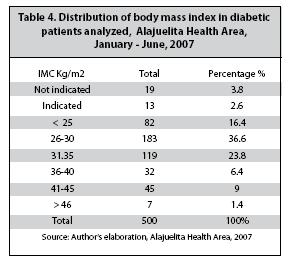
In table 4, the BMI
behavior of the sample of diabetic
patients from the Area can be seen; 3,8% of
the data
cannot be obtained, corresponding to patients for whom their BMI did
not appear
in the file. The BMI was calculated and interpreted for 96,25%.
Of the total sample analyzed, 183 patients (36,6%)
had
a BMI between 26-30. For
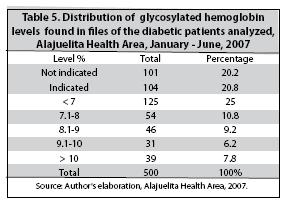
Measurement
of glycosylated
hemoglobin was not indicated at all for 110 patients (22%). It was
noted that
many times the AHA clinical laboratory did not meet the medical
indication for
an unknown reason. The glycosylated
hemoglobin level
was obtained for 43,6% of the sample; of
these, 125
patients (25% of the total) maintain an adequate level of HbA1c. 54
patients
(10,8%) had a HbA1c level between 7,1-8.
And
39 diabetic patients maintain a level >
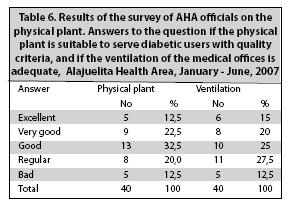
By
interviewing technical personnel, it was discovered
that 32,5% of the staff felt that the
physical plant
of the AHA is good; 22,5% said it was very good, and 20% said it was
normal. 30%
of the staff felt that the ventilation of the doctors and nurses
offices is
normal; 25% said it was good, and 17,5%,
that is very
good (Table 6).
Discussion
In Costa
Rica, DM is one of the non-transmittable
diseases whose prevalence is increasing and represents high costs for
social
security.5,6 The lifestyle changes of the population,
specifically
in dietary habits and physical activity, have conditioned an increased
incidence of chronic metabolic diseases and their complications. These
changes
affect the young population, which is experiencing an impact on some
specific morbities, such as DM.7-9
The two
techniques available for assessing management
effectiveness of glycemic control are the
measurement
of glucose and the HbA1c. The latter reflects blood glucose levels in
ten weeks
before, and has a strong predictive value for diabetic complications.
Furthermore,
it allows to corroborate the accuracy of
the results
reported by patient self-monitoring.
Glycosylated
hemoglobin (HbA1c) is useful for evaluating long-term control of DM; it
is a
complementary test to the fasting and postprandial glycemia.10 Its assessment can make the necessary adjustments
of the
treatment in order to achieve the international goal proposals for
adequate
control of diabetic patients and preventing complications.11
Clinical
indicators for monitoring diabetes mellitus
found in the cases studied in the AHA, provide an overview of the level
of
compliance with quality standards. It was found that the indication of
the
fasting glucose for patients is almost 100%, since the employees are
aware of
their importance for proper control in diabetic patients. Despite this,
the
indication for lipid profile percentage is relatively low (30%). It
also
emerged that the percentage of non-indication for HbA1c and other
parameters
required by MC by the AHA medical staff is low (22%).
It is
known by many that medical personnel in health
areas are very limited in time (15 minutes/ patient), and the MC
evaluates more
the filling of records than direct care and quality. An adjustment is
necessary
to relieve the medical staff of pressure from factors outside the MC.
This is
the first AHA study in its 10 years of
performance in the field of MC and care quality. The contribution made
in staff
perception of the Area, about the level of compliance with the quality
of care
provided to users, is important to verify treatment adherence, user
satisfaction and promotion of healthy lifestyles through the prevention
education program.
The
education program intended for users not only
promotes healthy lifestyle, it is also vital to prevent neurological
and nefrological complications (white
organ damage), the
suffering of patients and their close relatives, and to decrease the
health
service costs, since the complications involve high investment for
health
services and, consequently, a great social cost.
Alarmingly
more than one third part of the diabetic
sample had a BMI between 26 and 30 Kg/m2, indicating that
most
patients keep a range in between being overweight and having grade
I obesity. This alludes to carelessness on the users’ part, in their
ideal weight, probably reflecting the socioeconomic status and lower
levels of
education characteristic in the investigated community.
One
limitation of the study was not being able to
transcribe the perceptions regarding the received care, values and
expectations
of Health Area users, since their participation was excluded by the
lack of
knowledge regarding the disease, and low levels of education, as the
urban area
is marginal, and these perceptions not only depend on the medical team,
but
also the values and feeling of user and other external factors. It was
considered appropriate involve in the study the technical staff of the
Health
Area, since the information derived from the interview tends to be more
objective from their level of training with respect to the study,
making it
possible to access the actual services doctors in the area.
References
1. Sojo Ana. Reformas de gestión en salud en América Latina. Revista de CEPAL 2001,27:1-35
2. Sojo Ana. Hacia unas nuevas reglas de juego: los compromisos de gestión en salud de Costa Rica, desde una perspectiva comparativa. NUCEPAL 1998; 27: 118-140. [ Links ]
3. Miranda Gutiérrez, Guido. La seguridad social y desarrollo en Costa Rica. Segunda edición, San José: Editorial Nacional de Salud y Seguridad Social, 1994. [ Links ]
4. Barrantes E., Rodrigo. Un camino al conocimiento, un enfoque cuantitativo y cualitativo. II edición. San José, EUNED. 2006. [ Links ]
5. Calzada L.D. Diabetes mellitus tipo 1. En: Diabetes mellitus en Costa Rica. Primera ed. Laboratorios Stein, San José 2006; 89-99. [ Links ]
6. Morice A, Achio M. Tendencias, costos y desafíos para la atención de las enfermedades crónicas en Costa Rica. Rev Cien Adm Financ Seg Soc 2003; 11:18-34. [ Links ]
7. American Diabetes Association
8. Copeland k, Becker D, Gottschalk m, Hale D. Type 2 Diabetes in Children and Adolescents: Risk Factors, Diagnosis, and Clinical Diabetes 2005, 23:181-185. [ Links ]
9. American Diabetes Association. Type 2 Diabetes in Children and Adolescents. Pediatrics 2000:105:671-680. [ Links ]
10. Declaración de las Américas sobre
11. Sacks D, Burns D, Goldstein D, Maclaren N, Mc Donald J, Parrot M. Guidelines and recommendations for laboratory analysis in the diagnosis and management of diabetes mellitus. Clinical Chemistry 2002; 48:436-472. [ Links ]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}