










Serviços Personalizados
Journal
Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkActa Médica Costarricense
versão On-line ISSN 0001-6002versão impressa ISSN 0001-6012
Acta méd. costarric vol.54 no.3 San José Jul./Set. 2012
Original
Phenazopyridine:
A drug utilization research in the Costa Rican Social Security
Hugo Marín-Piva1, Carlos
Fonseca-Gamboa1, Desirée
Sáenz-Campos1, 2
Abbreviations:
ASSB,
Cartín”
Clinic; DDD, defined daily dosage;HCG,“
Dr. Rafael Angel Calderon Guardia” Hospital; UTIs,
urinary tract infection; LOM, official list of
medications.
Sources of support: Completion of this work did not receive external
economic
contribution of others, nor was under conflicts of interest with
pharmaceutical
companies or other.
Correspondence: carlos.cfg@gmail.com
Drug Area
and Therapeutics Clinic,
Department of Pharmacoepidemiology, Costa
Rican
Social Security.
Abstract
Background:
Phenazopiridine
is a urinary tract analgesic that has been deemed to be of low
intrinsic value;
nonetheless it has been used in the Costa Rican social security and has
a good record
of efficacy and safety within the institution.
Aim: To analyze
the use of phenazopiridine in the three
different
levels of attention in the Costa Rican social security.
Methods: During one
month, we obtained electronic pharmacy records from a first, second and
third
level health center to establish the quantitative characteristics of
the prescription
of phenazopiridine. For the qualitative
analysis a
random sample of 30 patients per center was generated; each file was
assessed
using a pre formulated instrument in order to review those patients’
files and obtain the required information.
Results: During the
month of January
Conclusion:
The use of
phenazopiridine is partially adequate, this
finding
supports the efficacy and safety in the context of attention in the
first and
second level centers. The diversity in the prescriptional
behaviors requires improvement by means of developing actions which
would
terminally
favor the rationality and therefore increase the impact of the benefit
offered
to the patients.
Keywords: phenazopyridine,
urinary tract infection, urinary antiseptics, dysuria,
drug utilization, rational drug use.
Phenazopyridine
is a urinary tract analgesic agent for oral administration. The drug is
described as a dye group “azo”, whose
chemical name is 2,6 diaminopyridine,
3 (phenylazo) Monohydrochloride.
In 24 hours, 90% is excreted in the urine, 41% as unchanged drug and
49% as
metabolites (most notably paracetamol),
which exert a
topical analgesic effect on the urinary tract mucosa.1
Based on
the principles of medicine based on evidence,
el analysis of the available scientific information showed the lack of
randomized clinical trials with the standard methodology of phase III
the lack
of systematic reviews with meth-analysis, to sustain the use of phenazopyridine as part of the management of
urinary tract
infections and other irritative syndromes.
Existing
information is scarce and of
poor
quality according to current standards required by scientific
publications.2-9
Despite
this, the drug is included in the Costa Rican
Social Security (CCSS) official list of medications (LOM), in
presentation of a
100mg tablet. Institutional experience of use of phenazopyridine
over 20 years, with a historical profile of safety and effectiveness,
and now,
the institutional consumption projected about 1830 patients who take
this
medicine every day, based on the daily defined dosage (DDD) 600 mg /
d10
orally, for its main indication as an analgesic for urinary tract
infections.1,
11
Under the
rational use of medications developed with Social
Security, the systematic and ongoing use of the drug in clinical
practice,
which contrasts with the weakness in the scientific information that
supports
the prescription, forms the basis for the study of drug use, in order
to
analyze the profile of phenazopyridine use
in the
context of routine clinical practice in outpatients, at different
levels of
attention and during a time period of 1 month.
Materials
and methods
In order
to meet this objective, an applied research
design, observational, analytical approach, and approval of the Central
Committee of the CCSS Pharmacotherapy for technology assessment in
health
studies paradigm drug use, according to the model
prescription-indication, we
proceeded at all times with a strict observation of the ethical
principles
confidentiality and non-malfeasance.
In
analyzing the use of phenazopyridine
in the context of clinical practice, as a first step the pharmacy was
requested
to release the drug during January
For
qualitative analysis of prescription medication on
a prescription-indication model, a random selection was made among all
cases of
drug clearance in each unit, during the period, seeking to have a
random sample
n = 30/unit. The sample size was defined for a minimum representation
of 20%
under the assumption of normality for compliance with the central limit
theorem.
With
emphasis on specific medical consultation that
supported the prescription drug, a selective review of the medical
records was
made, prior to endorsement of the medical departments of the units; in
a
predesigned form and without identifying individuals, the information
on
diagnosis, and age, dose, duration and other quantitative variables was
registered in an individualized way.
Data was
recorded and processed in an Excel ®
database for the initial descriptive statistical approach; tables and
figures
were designed, analytical phase of the results was developed and the
comparative analysis was drafted.
Results
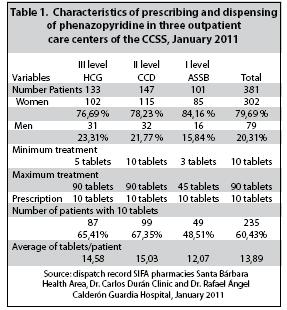
In the
course of one month, three medical units
dispatched 381 of the phenazopyridine
prescriptions
to patients seen, the vast majority of them, women; the prescription
varied in
the range of 3 to 90 tablets, although a high percentage of people (60,
43%) were
given prescriptions and only 10 tablets sent for treatment (Table 1).
Direct
information on the clinical use was available
in a considerable amount of medical records requested: 100% was revised
in
ASSB, 93% in the CCD and 93% in the HCG; but in the latter, only 8
cases (26%)
achieved the consultation document that generated the prescription.
Based on
the medical indication, it was possible to
systematize the annotation of the drug and the dose at 54, 55% of
cases. The
prescribed daily dose (PDD) was 100 mg TID, equivalent to 300 mg / d,
precisely
in half of patients; the second prescription scheme was 100 mg BID, in
33, 33%;
this profile with both dosages resulted uniform in the units of the
first and
second level of care. Other schemes prescribed were 200mg TID (5, 56%),
100mg
c/6h (5, 56%), 200 mg BID (2, 78%) and 100mg QD (2, 78%).
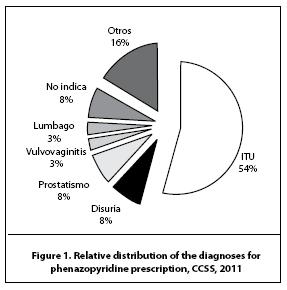
Phenazopyridine
was prescribed to 54,55% of patients with a
diagnosis
of urinary tract infection (UTI); amongst these, 89% were female
patients. It
was also prescribed for dysuria in 7,58% and for benign prostatic hypertrophy with prostatism in 7,58% (figure 1). In
addition, various causes
were recorded as the prescription of the drug to patients with the
following
conditions and diagnoses (n = 11, 16,67%): asymptomatic bacteriuria,
nonspecific urethritis, prostate cancer
detection,
gastroenteritis, gonorrhea, fever of unknown origin, urinary fixed
catheter,
transurethral resection of the prostate, kidney transplant, prostatitis
and renal cyst. The diagnosis for which the medication was prescribed
was not
written down by the prescriber in 7,58% of
the cases.
Regarding
diagnosis in 66 cases, using phenazopyridine
was associated with prescribing 89
additional drugs; 89% of patients diagnosed with UTI also received
antibiotic prescription.
The other four patients also received antibiotic prescription with phenazopyridine, were carriers of
asymptomatic
bacteriuria, nonspecific urethritis,
gonorrhea y prostatitis.
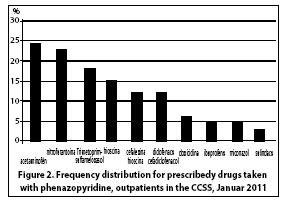
The
practice of associating drugs became more evident
in the second level of care, with the prescription of 46 drugs to 28
patients
(1,6 drugs / patient), the most commonly
prescribed
concomitant medication was acetaminophen with a 24,24%, followed by nitrofurantoin and trimethoprimsulfamethoxazole
with 18,18%, etc. (Figure
2); an additional prescription of ciprofloxacin, tramadol, metoclopramide
or dexamethasone, was recorded to 4
different patients.
The
duration of use, according to the number of dispensed
tablets, varied between 1 and 30 days. The most prolonged treatment was
recorded
at the units of second and third level care (90 tablet prescriptions).
In formal
terms, the treatment duration is recorded in less than half of the
cases (48,48%); the most common treatment
time was 3 days (43,75%),
followed by 5 (28,13 %) and 7 days (21,88%).
Discussion
This drug
utilization study, designed to evaluate the
usage profile of phenazopyridine in a
pattern of
prescription-indication, confirms that the drug is actually used as
part of the
management of urinary infections, which is attributed to its well known
analgesic properties. In addition, as part of this intervention, it is
validly
associated with causal antibacterial treatment; this therapy jointly
showed a
strong tendency towards rational use in the first and second level of
care.
An
important aspect of the findings emerged from this
work and based on a habit of prescribing, which also exceeds the
pharmaceutical
review for release of the medication, is the prescription of a
sub-therapeutic
dose of phenazopyridine, more than a third
of the
patients. According to available scientific evidence, it should be
remembered
that the dose for adults is 100 to 200 mg 3
times/day,
and for a period of
two days,
concomitantly with antibacterial treatment.5, 6,11
In
accordance with the principles of rational drug
use, the findings of this study show that most patients use the drug
for short
period, with the prescription of about 10 tablets per treatment,
primarily
indicated for the relief in the case of UTI, and with antimicrobials,
in the
case of UTI. This profile of the drug use is consistent with
international recommendations
for the clinical use of the drug, as to encourage prescribing for
patients with
a diagnosis of UTI, for 2 days of treatment, and concomitantly with an
antibiotic to resolve the ITU1, 5, 8, 11.
However,
in contrast to the above, it is unfortunate
that 11% of patients diagnosed with UTI, were not prescribed an
antimicrobial
agent. Moreover, it is noteworthy that phenazopyridine
is being prescribed to a variety of other diagnoses for which there is
no
scientific data to support its use in such conditions. The prescription
of the
drug, in such cases, it turns away from the principles of rational drug
use, to
nullify the benefit and maximize the inherent risks of the medication,
as would
be the occurrence of adverse effects. Similarly, the above
consideration of the
side effects, applies to the interactions derived from the frequent
combination
with other drugs. (acetaminophen,
non-steroidal antiinflammatories, hyoscine).
In the
medical files, prescribers documented various
diagnoses during consultation, which merited urinary analgesic
prescription and
lead to dubious rationality questionable practice to alleviate this
some degree
of urinary mucosal irritation, as a symptom associated in case of
gonorrhea,
prostatic pathology and vulvovaginitis;
however, no
valid pharmacotherapeutic information is
available to
support this practice.
Based on
information available from high-quality
scientific literature 2-9 and historical experience of
institutional
use, phenazopyridine is an effective
analgesic of
urinary mucosa, indicated for prescription for conditions with disuria and burning sensations, frequency and
urgency
associated with urinary tract infections, but without anti-infective
effect; so
it is imperative to note that during an ongoing infection, the
antimicrobial
agent is responsible for the final resolution, so that its prescription
should
not be omitted.
In
conclusion, by analyzing the usage profile of phenazopyridine
in the context of clinical practice at the
level of general and specialized outpatient medical care, in the
different
levels of care, for a period of one month, in the paradigm of the
principles of
rational drug use, the study findings show that the use is partial and
reasonably appropriate and, therefore, support the assumption of
effectiveness
for just over half of the patients, especially in the context of
medical care
in the first and second level of care, with a historical profile of
security. However,
the diversity in prescribing habits also highlights the need to improve
the
use, and it would be appropriate to develop actions to encourage more
rational
prescription, seeking to maximize the benefit for patients.
References
1. Sweetman S (ED), Phenazopiridine En: Martindale: The Complete Drug Reference.
2. Scottish Intercollegiate Guidelines Network (SIGN). Management of Suspected Bacterial Urinary Tract Infection in Adults: A National Clinical Guideline.
3.
4. European Association of Urology. Uncomplicated Urinary Tract Infections in Adults. Guidelines on Urological Infections. The Netherlands; 2008. [ Links ]
http://www.imedicinas.com/ GPTage/Search.php?text=fenazopiridina & searchButton=Buscar, consultado 28-06-2011. [ Links ]
6. Hadley S. Infecciones del tracto urinario. En: Rabel D. Medicina Integrativa. 2a ed. Barcelona: Elsevier-Masson, 2009: 259. [ Links ]
7. Hernández Fernández C, Verdú Tartajo F, de Palacio España A, González Chamorro F, Subirá Castejón C. Urgencias urológicas: cistitis aguda. Actas Urológicas Españolas. 1998, XIX (1): 11-18. [ Links ]
8. Rimsza ME, Kirk GM. Problemas médicos comunes del estudiante universitario. Pediartr Clin N Am 52(2005) 9-24. [ Links ]
9. Levy Hara G (Ed): Consenso intersociedades para el manejo de infecciones de tracto urinario, 2006. Recuperado el 28-06-2011 De: http://publicaciones.ops.org.ar/publicaciones/cursos_ virtuales/cursovirtualmedicamentos/dia4/bibliografia/sadi%20 consenso%20infeccion%20urinaria%202006.pdf
http://www.whocc.no/atc_ddd_ index/?code=G04BX06, consultado el 7-02-2011. [ Links ]
11. McEvoy G (ed). AHFS Drugs Information 2011. American Society of Health System Pharmacists. Bethesda 2011. [ Links ]
12. Caja Costarricense de Seguro Social. Sistema de Información Gestión de Suministros. Consultado en enero 2011. [ Links ]


{kind=link}
{kind=link}
{kind=link}