










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkActa Médica Costarricense
On-line version ISSN 0001-6002Print version ISSN 0001-6012
Acta méd. costarric vol.54 n.3 San José Jul./Sep. 2012
Original
Immune
status of patients with HIV/ AIDS at the time of diagnosis in the
Hospital San
Juan de Dios
Carmen
Vargas
Mejía1, Ricardo Boza Cordero1,2
Author´s
affiliation: 1HIV/ AIDS
Patient Care Clinic, San Juan de Dios Hospital, Caja
Costarricense de Seguro
Social
and 2 Universidad de Costa Rica´s
(University of Costa Rica) School of Medicine Abbreviations: LD, Late Diagnosis;HSJD,San Juan de Dios Hospital; HAART,
Highly Active
Antirretroviral Treatment; HIV,
Human
Immunodeficiency Virus
Correspondence:
cvarme@gmail.com
HIV/AIDS
Patient Care Clinic at San Juan de Dios
Hospital
Abstract
Aim:
To compare the immune status during three years of patients diagnosed
with
HIV/AIDS who were treated at the San Juan de Dios Hospital.
Materials
and Methods:
Retrospective, descriptive study of the new
cases of HIV/AIDS, older than 14 years of age, in 2003, 2006 and 2009
at the
HIV Outpatient Clinic of the San Juan de Dios Hospital,
Results:
From the 282 cases studied, 46.8% of them were at an advanced stage of
the
illness.
Considering
all cases, late diagnosis was more
frequent in men (54%) than in women (26%) (p<0.05) and in
heterosexual men
(57%) than in men who have sex with men (50%) (p<0.05).
In regard
to age, there is an increase in risk
proportional to the increase in age. It was observed that the
percentage of
late-diagnosis patients has increased throughout the years herein
studied. Even
though a decrease in the group of patients who come late for the start
of the
ART was observed, this decrease is due to an increase in late diagnosis
and not
because of an increase in timely diagnosis.
Conclusions:
Late diagnosis of HIV infection represents a public health problem in
the
geographical area covered by the services of the San Juan de Dios
Hospital. It
is necessary to develop strategies that allow the improvement of the
resolving
capacity of the primary and secondary levels of attention in order to
achieve
HIV diagnosis in a timely manner. In the geographical area covered by
the San
Juan de Dios Hospital, the populations with a greater risk of late
diagnosis
are heterosexual men between the ages of 25 and 64.
Key Words:
HIV, AIDS, CD4-positive T lymphocytes, late diagnosis,
immunodeficiency.
Human immunodeficiency virus (HIV) is a retrovirus that causes slow and progressive injury to the immune system; this is why people infected with the virus remain asymptomatic for several years, while continuous damage leads to severe immunosuppression, which could result in serious clinical consequences, favoring opportunistic infections and malignancies, potential causes of death for these patients. 1,2 In fact, the disease's natural is divided into theree stages: primary infection, which occurs after HIV infection with a significant viremia, and an intense immune response, wich could be a symptomatic stage: the second or chronic phase is a prolonged stage of clinical latency, characterized by continuous viral replication and progressive depletion of CD4+T lymphocytes (TCD4+) where patients often remain
Highly
Active Antiretroviral Therapy (HAART) has
allowed a change in this natural history, controlling viral replication
and
allowing immune recovery, resulting in a lower incidence of
opportunistic
infections and a lower mortality from HIV-related causes.4,5 Furthermore, scientific evidence has
shown that
continuous HIV replication is associated with a number of immune
defects that
cause irreversible immunosenescence. This
is why
various international guidelines recommend starting HAART at an immune
status
that permits a greater chance of recovering normal TCD4+ levels and
better
immune reconstitution, setting CD4 + <350 cells/ul
counts as a parameter. Some, more recent guidelines4-5 are even more
aggressive, recommending an earlier initiation of antiretroviral
therapy in
asymptomatic patients with TCD4 + counts between 350 and 500 cells/L,
based on
the damage caused by HIV infection in the untreated asymptomatic phase.5
These
results highlight the importance of early HIV
detection, so it is possible to initiate antiretroviral therapy in a
timely
manner, according to individual patient characteristics.
A late
diagnosis (LD), defined as the detection of new
infections with <200/μl
TCD4+ levels, means a higher risk of developing serious opportunistic
infections, drug-related adverse events and less immune recovery.6
Therefore,
early diagnosis becomes a key issue, not
just for an effective pathology approach, for the introduction of
antiretroviral therapy when it could reduce virus-associated
inflammation and
TCD4+ count depletion, but also in preventing and stopping
transmission,
allowing measures to prevent risky behaviors and decrease the infection´s transmissibility.7
For these
reasons, the immune status of patients presenting
with HIV/AIDS is analyzed, for those seen at HSJD for the first time.
Materials
and methods
A
descriptive, retrospective study was performed,
using medical records as a source of information.
All new
HIV cases diagnosed in 2003, 2006 and 2009
were analyzed, for those older than 14 years-old, treated at the HIV
Patient
Care Clinic at San Juan de Dios Hospital.
Immune
status at the time of HIV diagnosis is assessed
by using the TCD4+ lymphocyte count, defining late diagnosis as having
<200
TCD4+ cells/µ l.
All cases
diagnosed with HIV infection are included,
with two positive ELISA tests, and positive Western blot confirmatory
test, in
2003, 2006 and 2009. Patients who did not have an initial TCD4+count
determination were excluded.
Variables
analyzed included: age, gender, nationality,
sexual preference, TCD4+ lymphocyte counts.
Data
analysis was performed with SPSS 14.0, by
estimating the frequency and strength of association between variables.
Results
In the
analyzed period, 373 patients were identified;
91 were excluded because they did not have TCD4+ records, therefore,
the study
included a total of 282 patients (
{kind=link}
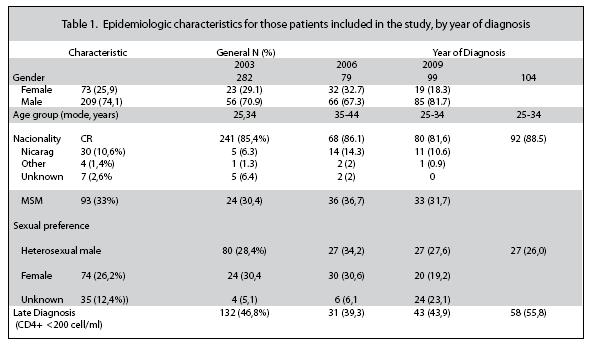
There were
more males in the study population, 74.1%;
mode was in the age group of 25-34 years. Foreigners corresponded to
12%, the
majority from
Regarding
the frequency of late diagnosis, for all
cases, analyzing the ratios, it was significantly greater in males
(54%) than
females (26%) (p <0.05), and in heterosexual men (57%) than in those
who
have sex with men (50%) (p <0.05).
Regarding age,
there is an increased risk of LD with increasing age.
Table 2
describes cases presented each year, according
to their TCD4+ levels, distributed in 3 groups: LD with advanced
disease (TCD4+
count <200 cells/ul),
late diagnosis to start HAART (CD4 counts between 200-350 cells/ul) and early diagnosis (TCD4+ count >350
cells/μl). The
percentage of patients with a late diagnosis increased over the studied
years;
even though the group of patients who arrived late for the start of
HAART
decreased, this was due to an increase in late diagnosis, not due to an
increase in early diagnosis.
{kind=link}
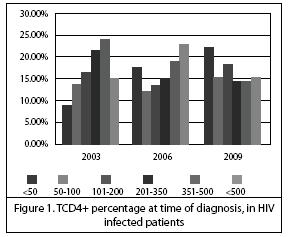
Figure 1
shows a more detailed distribution of
patients´ percentage, according to CD4 values at time of diagnosis. It
is
noteworthy how this chart shows a progressive increase not just for
patients
with late diagnosis, but with CD4 counts below 50 throughout the 3
years, and a
decrease in patients with early diagnosis.
Discussion
Early
HIV/AIDS diagnosis should be a key objective in
the
{kind=link}
In this
study, 46,8% of cases
presented at a late stage, or the stage of AIDS, meaning that these
patients,
according to this disease´s natural
history,
have carried the infection approximately 8 to 10 years, making this an
aggravating factor of the epidemic, as during this time they were
potential
infection transmitters, due to ignorance of their condition.
One
important aspect, seen in this study, is that the
percentage of late diagnosed cases has been increasing, mainly those
with TCD4+
<50 cells/μl,
resulting in a severe immune
Despite
the progress made in the field of HIV
diagnosis, achieving a shorter window period to four weeks, and the
fact that
Costa Rica has a health system that with a wide population coverage and
that
ensures the availability of tests in general, the study shows that late
diagnosis has increased over the years, and that early diagnosis has
decreased,
paradoxically. This could be related to a loss of awareness achieved at
the
beginning of the disease epidemic, both in the general population and
in the
health system, perhaps because “fear has been lost” to this illness
and basic aspects such as promotion, prevention and diagnosis have
become
unattended.15
In the
general population late diagnosis was lower in
women than men, similar to those reported in other countries,16
which may be related to the obligation, in our health care system, to
perform
two screening tests during pregnancy; another factor that could play a
role is
diagnosing women as part of contact tracing, but more studies are
needed to
support this specific evidence. However, during 2009 this ratio was
reversed,
and the highest proportion corresponded to late diagnosis in women.
Late
diagnosis gradually increased between ages 25 to
64, with a peak between 55 and 64, which reinforces the hypothesis of a
lack of
disease awareness and the absence of screening programs targeted at
risky populations,
because the test is performed until there is clinical evidence of the
disease.15
In the
male population there is a higher risk of late
HIV diagnosis for heterosexuals than for homosexuals, given a higher
risk
perception among men who have sex with men, associated with the stigma
that
this disease is more common among them.
The delay
in diagnosis may be due also to the lack of
clinical suspicion by health personnel. It is not uncommon to find
patients who
were treated in health centers several times, months earlier, because
of
illnesses clearly associated with HIV / AIDS, and who have not been
properly
diagnosed.
Although
it is not the aim of this study, it should be
noted that HIV / AIDS affects mainly in our environment, young people
between 25-40
years of age, who have unsafe sex with multiple partners, with homo
(40%) or
heterosexual (60%) behaviors, with a history of addiction to legal or
illegal
drugs in 40-50% of cases; 25% of these are women, 20% are commercial
sex
workers (Clinical HIV / AIDS HSJD, unpublished data).
Furthermore,
all patients with sexually transmitted
infections or tuberculosis should be studied for HIV/ AIDS. This should
also be
included in the differential diagnosis in patients with prolonged fever
(>
15 days), unexplained weight loss, cervical lymphadenopathy,
mononucleosis syndrome and cytopenias.
Multiple and
complex dermatologic manifestations could be seen for HIV / AIDS; for
women:
refractory vaginal candidiasis, cervical
dysplasia,
cervical cancer and pregnancy are mandatory conditions to study for HIV
/ AIDS.
There are excellent recent reviews on this topic.2,17
References
1. Fauci AS Lane HC Enfermedad por el virus de la inmunodeficiencia humana: Sida y procesos relacionados En: Braunwald E Kasper DL Longo DL Hauser SL Martin JB Fauci AS Jameson JL Loscalzo Jeditores. Harrison: Principios de Medicina Interna. 17 ed. México: Interamericana; 2009; 1137- 1203. [ Links ]
2. Cohen DE Mayer KH Primary care issues for HIV-Infected patients Infect Dis Clin N Am 2007;21:49-70
3. Miró J. M, Sueda O, Plan M, Pumarola T, Gallart T. Avances en el diagnóstico y tratamiento de la infección aguda por el VIH-1. EnfermInfeccMicrobiolClin 2004; 22:643-59
4.Panel on Antiretroviral Guidelines for Adults and Adolescents.Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents.Department of Health and Human Services.January 10, 2011; 1–166. En: http://www.aidsinfo.nih.gov/ContentFiles/AdultandAdolescentGL.pdf. [ Links ]
5. International AIDS Society-USA. When to start antiretroviral therapy. Top HIV Med. 2010; 18:121-126. [ Links ]
6. AlthoffKN Gange SJ Klein MB Brooks JT Hogg RS Bosch RJ et al.Late presentation for human immunodeficiency virus care in the
7. Joint United Nations Programme on HIV / AIDS (UNAIDS). Report on the Global AIDS Epidemic 2010 En:http://www.unaids.org/globalreport/Global_report.htm. [ Links ]
8. Castilla J Sobrino P De
9. Oliva J Galindo S Vives N Arrillaga A Izquierdo A Nicolau A et al. Retraso diagnóstico de la infección por el virus de la inmunodeficiencia humana en España. Enferm Infecc Microbiol Clin. 2010; 28: 583- 589. [ Links ]
10. The
11. Levu S Le Strat Y Barin F Pillonel J Cazein F Bousquet V et al Population- Based HIV-1 Incidence in France 2003-2008: a modelling analysis Lancet Infect Dis 2010;10:682-687
12. Art Cohort Collaboration HIV Treatment Response and Prognosis in Europe and
13. Keruly J. C, Moore R D. Immune Status at Presentation to Care Did Not Improve among Antiretroviral-Naive Persons from 1990 to 2006. Clin Infect Dis 2007; 45:1369–74. [ Links ]
14. Mojumdar K Vajpayee M Chauhan N Mendiratta SLatecpresenters to HIV care and treatment, identification of associated risk factors in HIV-1 infected Indian population. BSCPublic Health 2010, 10:416
15. Marks G, Crepaz N, Janssen RS. Estimating sexual transmission of HIV from persons aware and unaware that they are infected with the virus in the
16. Mugavero MJ Castellano C Edelman D Hicks C Late Diagnosis of HIV Infection: The Role of Age and Sex. Am J Med 2007; 120, 370-373. [ Links ]
17. Marco CA Rothman RE.HIV Infection and Complications in Emergency Medicine. Emerg Med Clin NAm 2008;26:367-387
 All the contents of this journal, except where otherwise noted, is licensed under a Creative Commons Attribution License
All the contents of this journal, except where otherwise noted, is licensed under a Creative Commons Attribution License

actamedica@medicos.cr