










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkActa Médica Costarricense
On-line version ISSN 0001-6002Print version ISSN 0001-6012
Acta méd. costarric vol.54 n.3 San José Jul./Sep. 2012
Original
Epidemiologic,
clinical, and microbiologic description of an outbreak of Clostridium
difficile associated diarrhea in Costa
Rica
Manuel Antonio Villalobos-Zúñiga1,
Ricardo Boza-Cordero2
Authors’
affiliation: 1Attending
Physician, Department of Infectious Diseases, San Juan de Dios
Hospital. 2 Attending Physician,
Department of Infectious
Diseases, San Juan de Dios Hospital. Associate
Professor,
Department of Infectious Diseases. San Juan de Dios Hospital, Caja Costarricense de Seguro Social.
Abstract
Background:
Clostridium
difficile associated
diarrhea (CDAD) is the main cause of nosocomial
diarrhea in the world.
Recently
there was an outbreak of CDAD in the San Juan
de Dios Hospital,
Population
and methods: A
CDAD case was defined as a patient with diarrhea and with
positive
ELISA for C. difficile A toxin in
feces. An
analysis of the annual incidence of CDAD from 2004 to 2008, and the
monthly
incidence in 2009 at HSJD was made, as well as a retrospective and
observational study of 112 medical records for patients diagnosed with
CDAD
treated at this hospital, from November 15, 2008 to June 15, 2009. The
analysis
of the data was made using descriptive statistics and measures of
association.
Results: The
incidence
of CDAD increased significantly since the end of 2008 and reached its
maximum
peak in April 2009, when sanitary measures were implemented. They
reduced by
75% the number of patients with CDAD in 8 months. Of the 112 medical
records
reviewed, 63 (56%) were men. The mean age was 65.33 years, 103 (92%)
patients
developed the disease while hospitalized; the mean period of
hospitalization
was 18.6 days. Only 9% did not suffer from any comorbidity.
The most
frequent comorbidities
were: hypertension and type 2 diabetes, with 57.5%
and 39.8%,
respectively, and neuropsychiatric disease with 29.2%. A 96%
(107
patients) had received three or more antibiotics before the onset of
diarrhea. The
mean duration of antibiotic therapy was 32 days per patient. In
average, the
duration of diarrhea was 10.2 days (1-90 days). Most patients were
treated with
metronidazole or vancomycin.
The mortality directly associated to CDAD was 7%.
implemented,
the impact was reduced in 75% over 8 months.
Key words: Diarrhea,
Clostridium difficile, outbreak, nosocomial infection.
Clostridium
difficile-associated
diarrhea (CDAD) is in the medical spotlight around the world, due to
the
constant outbreaks reported in the medical literature, with health,
economic
and scientific consequences. 1-3
C. difficileis an
anaerobic Gram-positive bacillus, that
forms spores
and produces cytotoxic toxins.It
is present in feces of less than 5% of the healthy adult population,
and 20-30%
of hospitalized patients are colonized by this bacterium during the
first week.1Due
to its ability to form thermostable
spores, it is not
easily eradicated from the hospital environment. Despite its discovery
in1935,
it was not until 1977 when it was linked to a medical condition,
pseudo-membranous colitis associated with the use of antibiotics, at
that
moment, with clindamycin.4
C. difficile is
the most frequent cause of acquired diarrhea in the hospital,
estimating tens
of thousands of cases per year around the world, with costs that
surpass one
billion dollars.5In the last decades there has been observed
an
important rise in the number of patients, due to improved diagnostic
methods,
an increased use of antibiotics and chemotherapeutic agents, as well as
a rise
in the number of sick persons, which increases the chance of
contamination by
spores in health centers, with a higher probability of infection in
susceptible
patients.6
The
gravity of the outbreak in
At the San
Juan de Dios Hospital (SJDH), in
Materials
and methods
The case
definition of CDAD was performed based on the presence
of diarrhea and a positive result for C. difficiletoxin
A in feces, detected by an ELISA assay. An analysis was performed of
annual
incidence of CDAD in San Juan de Dios Hospital, for adult patients,
with
approximately 700 beds since 2004, and in 2009 it was analyzed monthly.
Records
of 112 patients evaluated with a diagnosisof
CDAD
were studied, in the period between November 15, 2008 and June 15,
2009. It is
an observational, retrospective, descriptive and transversal study; the
Bioethics Committee of the medical center approved it.
The
following epidemiologic information of each
patient was analyzed: age; gender; address (province, canton and
district);
date of admittance to SJDH; date of diarrhea onset. Associated comorbidities and infections in all patients
were
registered and the hospital department where the diarrhea originated
was
consigned, as well as the type of antibiotic used and how long was it
used
before the diarrhea started. The following clinical variables were
collected:
record of daily stools, presence of abdominal pain, fever (it is the
highest
temperature value during the course of the disease), use of laxatives,
use of
drugs that modify gastric acidity, use of nasogastric
tube and history of recent surgery (in the last 3 months), leukocytosis,
bands percentage and serum albumin.
Initial
treatment for diarrhea was obtained: oral metrodinazole,
parenteral metronidazole,
oral vancomycin
125 mg o 500 mg every 6 hours, probiotic
agents, prebiotic agents, colestyramin
and immunoglobulin; and last, the suspension of “aggressor
antibiotics”; and the duration of these was indicated. Diarrhea
complications
were also documented: recurrence of the episode, toxic megacolon,
bacteremia, hydroelectric disorder, acute
renal
insufficiency, intestinal perforation, digestive bleeding, septic shock
and
other.
Regarding
recurrence of the episode, latency time was
Microbiologic
analysis was published previously.8
Data was
entered using Microsoft Office Excel
software, and for the statistical analysis, descriptive tests were
used.
Results
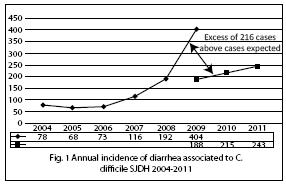
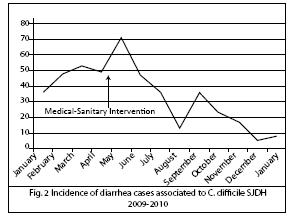
Incidence
of CDAD increased since November 2008 and
reached its peak in April 2009. An excess of 216 cases more was
expected with
respect of what was expected in 2009. With the measures taken in the
Hospital,
the number of new cases was reduced by 75% in the course of 8 months,
with a
monthly incidence below of that observed in previous years (Figs. 1 and
2).
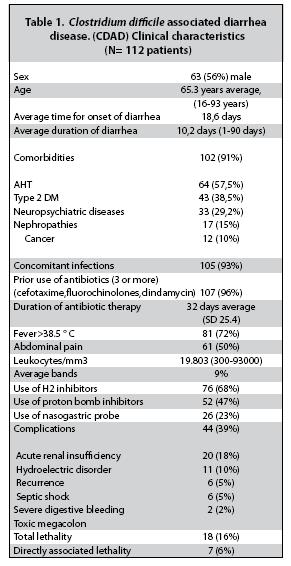
Out of 112
patients analyzed (Table
1), 63 were men
(56%). The mean age was of 65,33 years
(SD=16,63) and
the age range varied from 16 to 93 years.
Ten
patients developed the disease before their admittance,
or during the first day of this. The rest 112 patients (93%) were
diagnosed during
their hospitalization, and the average time of onset of the disease was
of 18,6 days, with a median of 14 and a mode
of 5 days.
On
average, the duration of CDAD was of 10,2
days (1-90 days).
71% of
patients were admitted to Internal Medicine
Department, 28% to the Surgery Department and 1% stayed in Emergency
Room.
Only 9% of
patients did not present any known comorbidity
at the time of diagnosis. Themost
common comorbidities were: HBP (high blood
pressure)
and Type 2 DM, with 57,5% and 39,8%
respectively. 29,2% of patients associated a
neuropsychiatric disease, among
the 4 most relevant: cerebrovascular event
(10%),
epilepsy (6%), depression (3%) and dementia (3%); other associated
conditions
were nephropathy with or without dialysis (15%) and cancer (10%).
Concomitant
infections were present in 105 patients
(93%) and were: 42% urinary tract infections (UTI), 34%
bronchopneumonia (BN),
25% skin and bland tissue infection (ISBT), 16% bacteremia,
6% infection of the superior respiratory tract (ISRT) and 1% infection
of the
central nervous system.
Only 5
persons (4%) had not received any antibiotic at
the moment of diagnosis; the rest (107,96%)
used at
least 3 different antibiotics before presenting the disease (two
patients
received 9 antibiotics and one received 11 different antibiotics).
The
average duration of antibiotic use was of 32 days
(1-96 days).
The three
most used antibiotics were: third generation
cephalosporin, ciprofloxacin, and clindamycin,
in
this order.
Fever was
present in 72% of patients. Abdominal pain
was present in 50% of those ill. The average leukocytosis
was of 19.803/mm3 (300-93000 cells/mm3). The average for immature
forms,
particularly bands, was of 9%. Near 60% presented hypoalbuminemia.
Moreover, 28% had a recent surgery history.
A 12,4% of patients had
received a laxative before the symptoms began; 46,9% had received
proton bomb
inhibitors (PBI) as antacid, and 68%, H2 receptor inhibitors. Only in
23% of
the patients a nasogastric tube(NGT)
was used.
The
treatment for the first episode was, in average,
of 13 days per patient.
An 87,5%
of patients received oral metronidazole
at a given time; 16% parenteral metronidazole;
25% oral vancomycin 125 mg every 6 hours,
and 5,3%
received oral vancomycin 500 mg every 6
hours. 58% of
patients received only one drug for the first episode of CDAD. As
alternative
treatments, probiotics were used in 6,25%, colestyramin
in 10%,
immunoglobulin in 3% and colectomy was
performed in
1%.
Regarding
complications, they were present in 93
patients (83%), and the most frequent ones were: acute renal failure
(ARF)
(39%), hydroelectric disorders (18%), sepsis (10%) or hypovolemic
shock(5%), severe gastrointestinal
bleeding(SGB) (5%),
bacteremia (3%), toxic megacolon
(2%) and one patient suffered colon perforation.
Eighteen
patients (16%) died and only 7 (6%) of those
cases by a direct effect of the CDAD; in 6 patients the diarrhea was
considered
a contributing cause of death and in 5 patients it did not have causal
relation.
Bacteriological
analysis was performed in 37 bacterial
isolates; all showed in vitro resistance to clindamycin
and fluorochinolones, and sensitivity to vancomycin and metronidazole;
54%
was of NAP1 type, positive for genes that codify for toxins A and B (tdcA, tdcB) and for
binary toxin
and with deletion of tcdC gene, which
regulates the
transcription of toxins.
Discussion
By the end
of the 90s, hospitals in different parts of
the world have been challenged with a new epidemic: the CDAD, which has
caused
great economic and health costs, even the closure of several clinics in
In the
study, the information of the Local Committee
for Prevention and Control of Infections of the SJDH allowed the
detection of
an unusual increment in the number of patients between November 2008
and April
2009. Between May and June of 2009, emergency health measures were
taken,
comprising, among other: development of protocols for patient care; strictisolation of affected patients in a
special unit;
promotion of hand-washing in health personnel; reduction in visits to
patients;
disinfection of hospital rooms, materials and equipment with
chlorinated
solutions; rationalization antibiotic use, as well as analysis of the
isolated
bacteria in a specialized laboratory.9
A
significant reduction in the number of patients was
achieved with these measures in a short time, and the complications and
lethality were similar and in some cases lower to those reported in
other
countries.10,11 For the first
time in Latin
America the strain of C. difficile NAP1
was
identified, responsible for this and other outbreaks in the world.3,8
Data
obtained through the study clearly evidences the
disproportionate affectation in the elderly, the average age is 65,33 years, and the median age 67 years. The
disease has a
tendency to affect preferentially persons older than 65 years, as
described in
the literature.2, 12-14 The CDAD is more aggressive in the
elderly,
with a higher relapse frequency, and they also present a lower response
to
treatment, the disease causes a prolonged hospitalization and, it also
is
associated to a higher mortality.14 The elderly population
has
several risk factors that make it particularly susceptible to C. difficile, like multidrug use with an extended
use of
antacids, antibiotics and laxatives, immunosenescence
and comorbidities, 12-14 not
considering
the continuous ethical dilemmas that some of these patients represent.
Comorbidities
of the patients are another risk factor and they describe this
population
accurately from a clinical -biological point of view, since 91% of the
sick
patients presented some associated pathology.
The HBP
and type 2 DM, were the most prevalent
pathologies, probably because the elderly predominate in the
population, among
whom the incidence is high; in fact, in many of the published studies,
these
two affectations occupy the first place in comorbidities
of the patients.16-18
It draw
the attention the fact that neuropsychiatric pathology
as comorbidity is not mentioned in the
literature,
with some emphasis, as a comorbidity in
CDAD; in this
study it showed, as important pathologies, cerebrovascular
disease, epilepsy, depression and dementia syndromes.
CDAD is
closely related with abuse in the use of
antibiotics.1,2,18-22 Among the undesirable effects of
these drugs
is the emergence of resistant bacteria, as well as the disturbance of
normal
bacterial flora, in these cases, intestinal flora´s
delicate equilibrium is altered by the indiscriminate use of
antibiotics and
there is elimination of fundamental bacteria for intestinal
homeostasis; so it
generates destruction of bacterial flora, that is proven with fecal
tests where
a decrease is found in these patients. This destruction allows the
proliferation of pathogenic bacteria, as C. difficile.
Most of the patients (91%) had received 3 or more antibiotics, among
which were
included third generation cephalosporins, fluorochinolones and clindamycin,
that have been related with this pathology.21-
Data from
the Pharmacy Department of the SJDH showed
that from 2007 to 2008 there was an increment of 49% in the use of cefotaxime, and of 23,5%
in levofloxacin, with similar projections
for 2009. An
inadequate use of antibiotics was documented in this analysis, in
quantity as
well as in duration of treatment. Even though, the indiscriminate and
irrational use of antibiotics is not the only risk factor for
developing CDAD,
it is one of the most important ones.
Prolonged
hospitalizations are also a risk factor for
CDAD, because patients have a higher risk of infection with this
bacteria, they
have a higher risk of exposure to antibiotics and other treatments; as
those
used to lower gastric acidity, which have already been associated with
the
pathology,18 as it is observed in this study. Again, it
should be
pointed out that most patients received antibiotics for very prolonged
times
while they were hospitalized.
Among
clinical manifestations, fever and abdominal
pain were the most frequent. Regarding fever, data should be analyzed
with
precaution, since it could be related with a concomitant infection.
Leukocytosis
is a common finding reported in the medical literature and it has been
related
with the severity of the infection, as well as hypoalbuminemia,
which was present in more than 60% of the patients.1,11,18 This
last
data can be associated with the loss of proteins due to the diarrhea,
because
it behaves as a protein-losing enteropathy.24
Of all the
patients, 31 (28%) had a history of recent
surgery in the past three months prior to the diarrheic episode, these
information reveals something very similar to what occurred in other
outbreaks,
like the one in Canada.16-24
Before the
emergence of this new strain, the treatment
for CDAD was relatively simple, where the suspension of the antibiotic
therapy,
the use of probiotics and the use of oral metronidazole for 5-7 days cured, practically
90% of the
patients, and the complications were less common and moderately severe.1-4
Since NAP1
has been related with this pathology, the
treatment is more complex, and the complications are more frequent and
more
serious,10,17,21 even
when some
authors doubt that the severity is exclusive to this strain. 11,18,19
In our
experience and according to the reports of
literature around the world,25,26 a consensus exists that
in
outbreaks where the hypervirulent strain
is involved,
patients must be treated aggressively from the onset, by using oral vancomycin for 2-3 weeks; these will lower the
duration of
the diarrhea as well as the complications associated with it. In some
cases,
intravenous metronidazole should be
associated, since
its bioavailability by oral administration in the intestine, is not
high
enough. With this study, it is not possible to elucidate which was the
best
therapeutic scheme, since it was a retrospective study.
The
importance of alternative treatments has been
discussed, for example probiotics,
immunoglobulin,
fecal bacteriotherapy, etc, however, only
the use of
immunoglobulin showed effectiveness, where an immunodeficiency is
demonstrated
in some patients with multiple recurrences.27,28 During the
outbreak, this therapy was used in three patients with satisfactory
results.
Regarding
the complications, they were similar to
those reported in the literature,2,5-7and it is noticeable
the there
is a low recurrence and lethality associated directly to this
pathology,
contrary to the popular perception externalized by the local media at
the time
of the incident.
Bacteriological
studies during this outbreak8 demonstrated
for the first time in
In
conclusion, in 2008 and 2009, an outbreak of CDAD
occurred in the SJDH, a hospital of 700 beds for adults, and the NAP1
strain
was identified, for the first time in
The
occurrence of such a multifactorial
and complex outbreak, as the one described in the present study, should
evidence the reality regarding the quality of the medical service
offered to
all the patients, and it should allow the identification of weak points
in our
everyday attention. Events like this one test the response capacity of
a
hospital and its human resource.
Acknowledgments
to Lic. Sandra
Araya Montero, member of
the Committee for Prevention and Control of Infections of the SJDH, and
to the
personnel of the Bacteriology Laboratory of the SJDH.
References
1. Thielman NM y Wilson KH. Antibiotic -Associated Colitis In Mandell,
2. Freeman J, Bauer MP, Baines SD, Corver, J Fawley WN, Goorhuis B et al. The changing epidemiology of Clostridium difficile infections. Clin Microbiol Rev 2010; 23: 529-549. [ Links ]
3. Clements ACA, Soares Magalhaes, RJ Tatem, AJ Paterson, DL Riley TV. Clostridium difficile PCR ribotype 027: assessing the risks of further worldwide spread. Lancet Infect Dis 2010; 10: 395-404. [ Links ]
4.
5. McDonald CL, Killgore GE, Thompson A, Owens RC, Kazakova SV, Sambol SP et al. An Epidemic, toxin gene-variant strain of Clostridium difficile N Engl J Med 2005; 353: 2433-2441. [ Links ]
6. Kelly CP y LaMont T. Clostridium difficile-more difficult than ever. N Engl J Med 2008; 359: 1932-1940. [ Links ]
7. Gravel D Miller, M Simor, A Taylor, G Gardam, M McGeer A et al. Health care-associated Clostridium difficile infection in adults admitted to acute care hospitals in
8. Quesada-Gómez, C Rodríguez, C Gamboa-Coronado, M Rodríguez-Cavallini, E Du T Mulvey MR et al. Emergence of Clostridium difficile NAP1 in Latin America. J Clin Microbiol 2010; 48: 669-670. [ Links ]
9. Gerding D,
10. Loo V Poirier, L Miller, MA Oughton, M Libman, MD Michaud S. A predominantly clonal multi-institutional outbreak of Clostridium difficile-associated diarrhea with high morbidity and mortality. N Engl J Med 2005; 353: 2442-2449. [ Links ]
11. Hookman P y Barkin J. Clostridium difficile associated infection, diarrhea and colitis. World J Gastroenterol 2009; 15: 1554-1580. [ Links ]
12. Jagai J y Naumova E. Clostridium difficile-associated disease in the elderly.
13. Zilberberg MD, Shorr AF, Micek ST, Doherty JA y Kollef M H. Clostridium difficile-associated disease and mortality among the elderly critically ill. Crit Care Med 2009; 37: 2583-2589. [ Links ]
14. Diggs NG y Surawicz CM. Clostridium difficile infection: still principally a disease of the elderly. Therapy 2010; 7: 295-301. [ Links ]
15. Cober ED y Malani P N. Clostridium difficile infection in the “oldest” old: clinical outcomes in patients aged 80 and older. J Am Geriat Soc 2009; 57: p 659-662. [ Links ]
16. Raveh D, Rabinowitz B, Breur GS, Rudensky B y Yinnon AM. Risk factors for Clostridium difficile toxin-positive nosocomial diarrhea. Int J Antimicrob Agents 2006; 28: 231-237. [ Links ]
17. Pépin J, Valiquette L y Cossette B. Mortality attributable to nosocomial Clostridium difficile-associated disease during an epidemic caused by a hypervirulent strain in Quebec. CMAJ 2005; 173: 1037-1042. [ Links ]
18. Suneshide RH y McDonald LC. Clostridium difficile-associated disease. New challenges from an established pathogen. Clev Clin J Med 2006; 73: p 187-197. [ Links ]
19. Blondeau J M. What have we learned about antimicrobial use and the risks for Clostridium difficile-associated diarrhoea? J Antimicrob Chemother 2009; 63: 238-242. [ Links ]
20. Weiss K, Bergeron L, Bernatchez H, Goyette M, Savoie M y Thirion D. Clostridium difficile-associated diarrhoea rates and global antibiotic consumption in five Quebec institutions from 2001 to 2004. Int J Antimicrob Agents 2007; 30: 309-314. [ Links ]
21. Owens RC, Donskey CJ, Gaynes RP, Loo VG y Muto CA. Antimicrobial-associated risk factors for Clostridium difficile infection. Clin Infect Dis 2008; 46: S 19–31. [ Links ]
22. Pépin J, Saheb N, Coulombe MA, Alary ME, Corriveau SA, Leblanc M et al. Emergence of fluoroquinolones as the predominant risk factor for Clostridium difficile-associated diarrhea: a cohort study during an epidemic in
23. Saxton K,
24. Efron P y Mazuski J E. Clostridium difficile colitis. Surg Clin N Am 2009; 89: 483-500. [ Links ]
25.Bartlett JG.The case for vancomycin as the preferred drug for treatment of Clostridium difficile infection.Clin Infect Dis 2008;46: 1489-1492. [ Links ]
26. Cohen SH, Gerdin DN, Johnson S, Kelly CP, Loo V McDonald CL et al. Clinical practice guidelines for Clostridium difficile infection in adults: 2010 update by the Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA). Infect Control Hosp Epidemiol 2010; 31: 431-455. [ Links ]
27. Aslam S, Richard J, Hamill RJ y Musher DM. Treatment of Clostridium difficile-associated disease: old therapies and new strategies. Lancet Infect Dis 2005; 5: 549–57. [ Links ]
28. Wilcox MH. Descriptive study of intravenous immunoglobulin for the treatment of recurrent Clostridium difficile diarrhea. J Antimicrob Chemother 2004; 53: 882–884. [ Links ]


{kind=link}
{kind=link}
{kind=link}