










Servicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkActa Médica Costarricense
versión On-line ISSN 0001-6002versión impresa ISSN 0001-6012
Acta méd. costarric vol.54 no.3 San José jul./sep. 2012
Original
Hypovitaminosis D
in
Chih Hao
Chen-Ku1, Manuel Jiménez-Navarrette2, Laura Ulate Oviedo2
Authors´
affiliation: Department of
Endocrinology, San Juan de Dios´ Hospital. Department of Clinical
Pharmacology and Toxicology, University of Costa Rica.1 Department
of Endocrinology, San Vicente de Paúl
Hospital, Heredia2
Abbreviations:
25(OH) VD;
25-Hydroxi-vitamin D; BMD, Bone mineral density; USA; United States of
America;
UVI, Ultraviolet index; PTH, Parathormone;VD,Vitamin
D.
Department of Endocrinology, San Juan de Dios Hospital
Abstract
Aim: To
describe for the first time clinical characteristics of patients with
vitamin D
insufficiency in
Materials
and methods: 17
patients with low levels of 25(OH)VD (<75
nmol/L) were selected from the laboratory
reports at the
Hospital San Juan de Dios. 15 controls were selected with normal 25(OH)
VD
levels and the same age and gender.
Results: There was
no difference in age (52.76±20.88 years in cases vs
46.33±
Conclusions:
Vitamin D
insufficiency may present even in tropical countries such as
Key words: vitamina D deficiency, vitamina
D, hyperparathyroidism
The
vitamin D (VD) really is a hormone that is
produced by the skin, mainly thanks to the exposure of the solar
Ultraviolet B
rays and in less degree, by food sources and diet supplements. The
active
metabolite 1,25-dihidroxy-vitamin D
(25(OH)VD) and the
parathyroid hormone (PTH), are the principal regulatory hormones of
calcium and
both influence on its synthesis mutually.1
Hypovitaminosis
D is a public health topic recognized worldwide, with different
variability in
its prevalence, according to geographic areas. It is a pandemic
problem,
principally provoked by having less sun exposure on the human being and
the
inadequate supplementation of this hormone through food. Even in
regions of
high exposure, like Hawaii (USA) and
VD
insufficiency provokes rickets in children and osteopenia
and osteoporosis in adults. However, in the last
years have been described more often the correlation of this deficit
with extra
skeletal effects, like increase risks of various cancer, diabetes
mellitus type
1, multiple sclerosis, Rheumatoid arthritis, acute myocardial
infarction and
arterial hypertension.4,5 American
NHANES
III results, show an increase of total mortality when the 25(OH) VD is
less
than 44,5 nmol/L.6
Prevalence
of insufficient and deficient of 25(OH) VD
have also been found in populations apparently healthy, in all ages and
in
different geographic latitudes, that predisposes to future pathologies
compromising their quality of life.7,8
The
Ultraviolet index (UVI) is a diary forecast, calculated
and divulgated with anticipation of 24 hours, the amount of ultraviolet
radiation received by the Earth´s surface
for
most solar lighting, usually located around afternoon. It is a measure
of
guidance aimed at promoting healthy sun exposure, skin photo type
adjusted in
each person. It’s indicated the ultraviolet radiation levels on a scale
of 1 (low) to >11 (dangerously high)
From the
different VD molecules that are found in the
human body, the 25(OH)VD in plasma is considered VD status ¨mirror
image¨ of a person, because it reflex the sum of the VD absorbed in the
intestine and the level produced in the dermal. If well this molecule
is
biologically inactive, many research have found that the determination
of serum
levels constitute an important determinant of multiple biological
functions, including
the bone and muscular mineralization.12-14
Several
studies have evaluated 25(OH) VD different
concentrations relative to bone density, lower extremity function,
dental
health, as well as high fall risks, fractures and colon cancer. The
most accepted
definition of optimal concentration of this hormone is advocated that
the PTH
levels above which the latter exerts deleterious effects on the body,
mainly in
the bone metabolism, is about 75nmol/L.15
Hypovitaminosis
D is the condition that occurs when the 25 (OH) VD levels are lower
than
75nmol/L(30 ng/ml),
and its
subdivided in two groups: insufficiency (levels between 51nmol/L to 74 nmol/L; 21-29 ng/mL)
and
deficiency (lower levels of 50 nmol/L;<20
ng/ml).16-18
In 2007
began measuring levels of 25(OH) VD at the
Hormonal Laboratory at San Juan de Dios Hospital, only center in Costa
Rican
social security leading of that determination.
The object
of this study is to describe, for the first
time in
Methods
and Materials
Retrospective
study of 1 year
(January to December, 2008). The Hypovitaminosis
D was defined as levels less than 75 nmol/L
(30 ng/ml). Was
selected 17 patients under those levels and 15 normal controls.
Was
analyzed the clinical Files of a 32 persons sample, and was recollected
demographic and clinical characteristics, like fractures, diabetes
mellitus,
history of cardiovascular diseases and previous use of medication. The
sample
was contacted to find out the sun exposure (hours per week), previous
use of sunblock and associated symptoms.
The vitamin D levels were
requested by the attending physician as part of their studies in
clinical
evaluation for various conditions.
The 25(OH)
VD was measured at the Hormonal Laboratory
of San Juan de Dios Hospital, by mean of ELISA test, using the reactive
kit IDS
Octeia. The sample has been taken in
fasting. The
statistical analysis that were held using the SPSS 15 package; the continues variables were analyzed using the
T-student
prove and the chi-square categories.
The study
was approved by the Local Bioethics
Committee of the San Juan de Dios Hospital.
Results
Was
identify 17 carriers cases of Hypovitaminosis
D and 15 controls were chosen. The average age of the cases group were
52, 76
± 20,88 years and the group control 46,33
± 12,50(p=0,307). Females were predominant in both groups, with 58, 8%
for cases and 80% for controls (p=0,265).
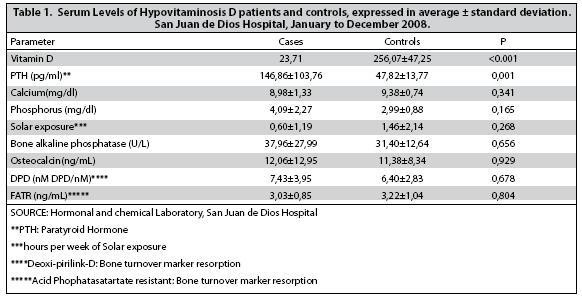
The
laboratory findings, the 25 (OH) VD average level
was 59, 2 ± 10,37 nmol/L
(23,71 ng/ml) was between insufficient;
the PTH was
found high between Hypovitaminosis D
carriers
(average 146,86 pg/mL vs. 47,82 pg/mL controls, p 0,001). Over the other
biochemical
parameters, there were no significant differences (Table 1).
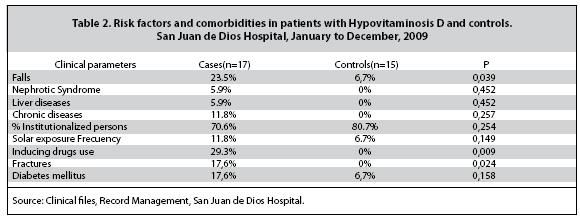
On risk
factors and comorbidities,
the 25(OH)VD insufficient showed more weakness (41,2% vs. 33% of
controls;
p=NS), osteoporosis (35,3% vs. 7% of controls, p<0,001), fatigue
(29,4% vs.
13% of controls; p=0,098), falls (23,5% vs. 7% of controls;
p=0,039),fractures
(17% vs. 0% of controls; p=0,024), diabetes mellitus type 2 (17% vs.
6,7% of
controls; p=0,158), and used sunscreens (11,8% vs. 7% of controls) (table 2).
Discussion
The 1,25 (OH)2 Vitamin D is
the active form of this hormone. Contrary to logical thinking, the Hypovitaminosis D is not defined by low levels
of this
active form of the vitamin, but the 25 (OH) Vitamin
D.
This is because when the 1,25(OH)2 Vitamin D
levels
decreases, secondary hyperparathyroidism occurs. The increased activity
of PTH
stimulates the action of the 1-α-hydroxylase, which
catalyzes the 25(OH) Vitamin D conversion to 1,25(OH)2
Vitamin D. In these circumstances, it would have a ¨normal¨ false level
of 1,25 (OH)2 vitamin D, at the expense of
secondary
hyperparathyroidism. Measure 25 OH Vitamine
D obvious
these considerations.19
Despite
the abundant solar exposure, the prevalence of
Hypovitaminosis D is high among populations
of
regions with much sun exposure, like Hindus and South Asians, in which
can
reach the 97% of prevalence.20 The lack of adequate sun
exposure is
a risk factor to present Hypovitaminosis
D. The study
identified a trend to low amounts of this hormone, although not
statistically
significant.
It is to
emphasize the value obtained from one
exposure of 0,6hours per week of sunlight, equivalent to only 5 minutes
a day.
That value is low, despite being a tropical country with abundant
sunshine
during the all year. Some lifestyle changes explain this finding. Today
it was
increased awareness about prevention of skin cancer, so people tend to
receive
less direct sunlight. Furthermore, the type of work has affected the
population, a high percentage, if covered for most of the day. All this
contributes to that the sun exposure is on average much lower than
recommended,
at least 15 minutes per day.21-23
Another
factor not identified until recently, which
may help to explain the high Hypovitaminosis
D, is
the contribution of genetic factors. Different genes Polymorphisms
involved in
the VD synthesis, transport and action, are associated with relative
risks 2,5 times more likely to have Hypovitaminosis
D.24
Females
are another risk factor for Hypovitaminosis
D, and in this study, 80% of the women
affected. Furthermore, their carriers of both genders have more history
of
fatigue, osteoporosis, falls, fractures, diabetes mellitus and liver
enzyme
inducing drugs.
The liver
and renal diseases, institutionalized
persons, the elderly, mal absorption syndromes, pregnancy, lactation
and use of
anticonvulsant drugs, are considered risk factor for Hypovitaminosis
D.25 In the presence of renal insufficiency; the
1-hydroxylase
activity is less, so there is a lower activation of Vitamin D, leading
to
secondary hyperparathyroidism. In this research, the only statistically
significant risk factor was the use of
hepatic-enzyme induce
drugs.
It was
also found high prevalence of musculoskeletal
symptoms and signs, like fatigue, weakness, osteoporosis and fractures.
A
quarter of the patients have fall history, which increases fractures
risk. No
differences were found between the case and the control groups with
respect of
the use of sunscreen and weakness. The VD has genomics and no genomics
effects
to muscle fiber. It has been shown that deficiency states, there is
muscular
fiber atrophy type II, which are rapid response and the first to be
recruited
to prevent falls. Some studies have shown reductions of up to 20% on
risk of
falls when correcting the VD deficiency, which may contribute to anti
fracture
efficacy has been determinate.26
Although
not assessed in this study, the extra
skeletal effects of VD are multiples. Different bibliographic sources
correlate
VD levels to cancer prevalence,27
worsening
insulin resistant getting and glycemic
control,28
more prevalence of autoimmune diseases like diabetes mellitus
type 1 and
multiple sclerosis. Even some early studies have shown that
supplementation
before the first year of live is associated to a low risk to developed
diabetes
mellitus type 1 during childhood.29
This study
has several limitations. The first one is
that the sample is small, which may explain why the differences not
reach
statistical significance in many international risk factors associated
to VD
deficiency. However, is the first Hypovitaminosis
D
report in
More
research is required to know the real prevalence
of this condition in
References
1. Holick MF, Chen TC. Vitamin D deficiency: a worldwide problem with health consequences. Am J Clin Nutr 2008; 87 (Suppl): 1080S-86S. [ Links ]
2. Binkley N, Novotny R, Krueger D, Kawahara T, Daida YG, Lensmeyer G, Hollis BW, and Drezner MK. Low Vitamin D Status despite Abundant Sun Exposure. J Clin Endocrinol Metab 2007; 92: 2130–35. [ Links ]
3. Bandeira ZF, Griz L, Freese E, Castro-Lima D, Thé AC, Trovão-Diniz E, Fontenele T, Salgado C. Vitamin D deficiency and its relationship with bone mineral density among postmenopausal women living in the tropics. Arq Bras Endocrinol Metab. 2010;54(2):227-32. [ Links ]
4. Bikle D. Nonclassic Actions of Vitamin D. J Clin Endocrinol Metab 2009; 94: 26–34. [ Links ]
5. Giovanucci E, Lui Y, Hollis BW and Rimm EB. 25-Hydroxivitamin D and Risk of Myocardial Infarction in Men. Arch Intern Med 2008; 168 (11): 1174-80. [ Links ]
6. Michos ED, Melamed ML, Post W,
7. Calatayud M, Jódar E, Sánchez R, Guadalix S y Hawkins F. Prevalencia de concentraciones deficientes e insuficientes de vitamina D en una población joven y sana. Endocrinol Nutr 2009; 56 (4): 164-9. [ Links ]
8. Steingrimsdottir L,Gunnarsson,O,Indridason OS, Franzson L and Sugurdsson G. Relationship Between Serum Parathyroid Hormone Levels, Vitamin D Sufficiency, and Calcium Intake. JAMA 2005; 294: 2336-41. [ Links ]
9.Instituto Geográfico Nacional de Costa Rica. Aspectos geográficos. http://www.mopt.go.cr/ign/IGN-Aspectos-Geográficos.html. Consultado junio de 2010. [ Links ]
10. Instituto Meteorológico Nacional (Costa Rica). ¿Qué es el índice ultravioleta? http://www.imn.ac.cr/educacion/UV/UVMAS2. html,consultado durante el mes de junio del 2010. [ Links ]
11. Instituto Meteorológico Nacional (Costa Rica). Mapa del índice ultravioleta máximo por regiones climáticas del país. http://www.imn.ac.creducacion/UV/INDICEUV.html, consultado en marzo de 2010. [ Links ]
12. Rejnmark L, Vestergaard P, Heickendorff L and Mosekilde L. Plasma 1,25(OH)2D levels decrease in postmenopausal women with hypovitaminosis D. Eur J Endocrinol 2008; 158: 571-76. [ Links ]
13. Holick MF. The vitamin D epidemic and its health consequences. Journal of Nutrition 2005; 135: 39S-48S. [ Links ]
14. Bischoff-Ferrari HA, Giovannucci E, Willet WC, Dietrich T & Dawson-Hughes B. Estimation of optimal serum concentrations of 25-hydroxivitamin D for multiple health outcomes. American Journal of Clinical Nutrition 2006; 84: 18-28. [ Links ]
15. Bischoff-Ferrari HA, Giovannucci E, Willett WC, Dietrich T and Dawson-Hughes B. Estimation of optimal serum concentrations of 25-hydroxyvitamin D for multiple health outcomes. Am J Clin Nutr 2006; 84:18 –28. [ Links ]
16. Chapuy MC, Preziosi P, Maamer M, Arnaud S, Galan P, Hercberg S et al. Prevalence of Vitamin D insufficiency in an adult normal population. Osteoporosis Int 1997; 7: 439-43. [ Links ]
17. Malabanan A, Veronikis IE, Holick MF. Redefining vitamin D insufficiency. Lancet 1998; 351: 805-6. [ Links ]
18. Dawson-Hughes B, Heaney RP, Holick MF, Lips P, Meunier PJ, Vieth R. Estimates of optimal vitamin D status. Osteoporosis Int 2005; 16: 713-16. [ Links ]
19. Binkley N, Ramamurthy R, Krueger D. Low vitamin D status: definition, prevalence, consequences and correction. Endocrinol Metab Clin N Am. 2010; 39: 287-301. [ Links ]
20. Zargar AH, Ahmad S, Masoodi SR, Wani AI, Bashir MI, Laway BA, Shaz ZA. Vitamin D Status in Apparently Healthy Adults in
21. Rajakumar K, Greenspan SL, Thomas SB, and Holick MF. Solar Ultraviolet Radiation and Vitamin D. An historical perspective. Am J Public Health; 2007; 97: 1746-54. [ Links ]
22. Carbonea LD, Rosenbergb EW, Tolleyc EA, Holick MF, Hughesb TA, Watskye MA, Barrowb KD, Chend TC, Wilkinb NK, Bhattacharyab SK, Dowdyf JC, Sayreb RM, Weber KT. 25-Hydroxyvitamin D, cholesterol, and ultraviolet irradiation. Metab Clin Exper; 2008; 57: 741–748. [ Links ]
23. Chel VGM, Ooms ME, Popp-Snijders C, Pavel S, Schothorst AA, Meulemans CCE and Lips P. Ultraviolet Irradiation Corrects Vitamin D Deficiency and Suppresses Secondary Hyperparathyroidism in the Elderly. J Bone Miner Res 1998;13:1238–1242. [ Links ]
24. Wang TJ, Zheng F, Richard B, Kestenbaum B, van Meurs JB, Berry D et al. Common genetic determinants of vitamin D insufficiency: a genome wide association. Lancet. 2010. Publicado en línea 10 de junio 2010. DOI:10.1016/S0140-6736(10)60588-0. [ Links ]
25. Lee JH, O’Keefe JH,
26. Binkley N, Ramamurthy R, Krueger D. Low vitamin D status: definition, prevalence, consequences and correction. Endocrinol Metab Clin N Am. 2010;39:287-301. [ Links ]
27. Krishnan AV, Trump DL, Johnson CS, Feldman D. The role of vitamin D in cancer prevention and treatment. Endocrinol Metab Clin N Am. 2010;39:401-418. [ Links ]
28. Takiishi T, Gysemans C, Bouillon R, Mathieu C. Vitamin D and diabetes. Endocrinol Metab Clin N Am. 2010;39:419-446. [ Links ]
29. The EURODIAB Substudy 2 Study Group. Vitamin D supplementation in early childhood and risk for type 1 (insulin dependent) diabetes mellitus. Diabetologia. 1999;42:51-4. [ Links ]


{kind=link}
{kind=link}