










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkActa Médica Costarricense
On-line version ISSN 0001-6002Print version ISSN 0001-6012
Acta méd. costarric vol.54 n.2 San José Apr./Jun. 2012
Comunicación breve
Etiological
agents of onychomycosis diagnosed in the
medical
mycology laboratory of the
Ingrid
Salas-Campos, Norma T. Gross-Martínez
Sección
de Micología Médica,
Facultad de Microbiología,
Universidad de Costa Rica
Abstract
Background
and aim: Among the onychodistrophies,
onychomycosis are the most frequently
encountered. This
infection not only constitutes an esthetic problem for the patients,
but can
also affect their daily activities. For dermatologists, it is crucial
to make a
differential diagnosis; thus, the medical mycology laboratory plays an
important role to achieve this purpose. The fungal agents most
frequently
encountered are the dermatophytes,
however, other filamentous
non dermatophyte fungi have been isolated
and are
known to be less susceptible to antifungals.
In the present work, 115.
The
frequency of onychomycosis
among patients attending the medical mycology laboratory, UCR, was
studied
during four years, according to the age and sex of the patients, as
well as the
isolated etiological agents identified.
Methods:
The study included all patients that requested the community service
provided
by the Department of Medical Mycology,
Results:
A total of 431 nail samples were collected, of which 85.4% were
toenails and
14.6% fingernails. The mean age of the patients was 49 years, of which
64% were
females and 36% males. Onychomycosis was
diagnosed,
either by direct microscopy and culture, or only with positive direct
microscopy, in 73.4% of the sample population, of which 89.4% were
toenails and
10.6% fingernails. Trichophyton rubrum was the etiological agent most
frequently
isolated from toenails, followed by Fusarium
spp. C albicans was the most
frequent
fungal agent observed in fingernails.
Conclusion:
The diagnosis of onychomycosis relies upon
both the
clinical and laboratory diagnosis. Dermatophytes,
yeasts and non-dermatophyte filamentous
fungi were
identified in the population studied. These findings should be
considered due
to their implications to the choice of the most appropriate treatment.
Key words:
onychodystrophies, onychomycosis,
dermatophytes, filamentous non dermatophyte
fungi.
A
complication of onychomycoses
is the difficulty of their treatment because of the rate of therapeutic
failure, which ranges from 20-50%.3 For
the
dermatologist it is necessary to make a differential diagnosis of nail
diseases
and that is why the Medical Mycology laboratory plays a central role
assisting
this process. It is not only necessary to recognize that the condition
is an onychomycoses, but also to be able
to identify the
etiologic agent involved because for non-dermatophyte
filamentous fungi recently described in Costa Rica4,5
a priori prescription is not possible since some of these
fungi,
such as Fusarium, are resistant to
imidazoles6,7,
while for others, such as Scytalidium dimidiatum, there is
no efficient treatment.8 This
situation makes necessary to look for other therapeutic options.
Onychomycoses
are not only an aesthetic problem for the patient, but they can also
affect
daily activities such as walking, standing, exercising, recreation,
nail
trimming, and even shoe preference because of the appearance of their
nails if
wearing sandals or the microenvironment and the thickening of the nails
when
wearing closed shoes.10,11 This infection’s effect on the
appearance
of nails can also alter the patients’ psychological status by inducing
shame, low self-esteem, anxiety and social effects among others.9,10
It can also cause complications in elderly diabetic or vascular
disease-affected patients, such as cellulitis9,12, and even
systemic
dissemination of the fungi from nails in immunocompromised
patients.2,13
In this
study, we analyzed the frequency of onychomycoses
that were diagnosed at the Medical Mycology
laboratory of the University of Costa Rica
(UCR)
during 4 years and classified by patient age and gender, as well as the
etiologic agent that was identified.
Methods
This study
included all the samples from patients with
ungual lesions that were received for
examination on
the suspicion of onychomycoses between
January 2007
and December 2010 as part of the service provided by the Medical
Mycology
Section of the Faculty of Microbiology, project ED-539 of the Social
Action
Vice rectory, UCR. For each patient, name, age and gender were
recorded, and
then a sample of subungual detritus or, if
there was periungual inflammation, a
sample of the affected tissue
was obtained. All samples were examined by direct observation in 40%
KOH and
fungal elements were searched for under the microscope. Part of the
material
was cultured on Saburaud’s agar and media
with actidione and chloramphenicol.
Cultures
were incubated at room temperature for at least 15 days. The
identification of
filamentous fungi was based on macroscopic and microscopic
characteristics of
the colony while the identification of the yeasts was carried out with
metabolic tests including the semi-automated API system or an automated
Vitek®.
Results
During the
study’s period a total 431 nail
samples were processed. Of these, 85.4% were toenails, and the
remaining 14.6%
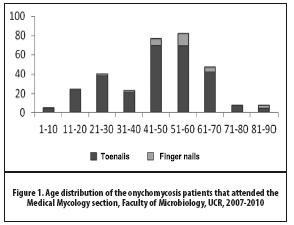
were fingernails. Patient’s mean age was 49 years (range 5-87 years;
Figure 1) and 64%
of them were female and 36% male.
Among the
samples, 119 (27.6%) had a negative result
for fungi in both the direct examination and the cultures. In the
remaining 312
samples (73.4%) a diagnosis of onychomycosis
was
established by either direct examination, culture or both, of which 279
(89.4%)
were toenails and 33 (10.6%) were fingernails.
Among the
279 toe onychomycoses,
122 (43.7%) were from males and 157 (56.3%) from females. Age
distribution of
these samples is shown in Figure 1. For 273 samples (97.8%) the direct
examination was positive, 135 (48.4%) of which had negative culture
while from
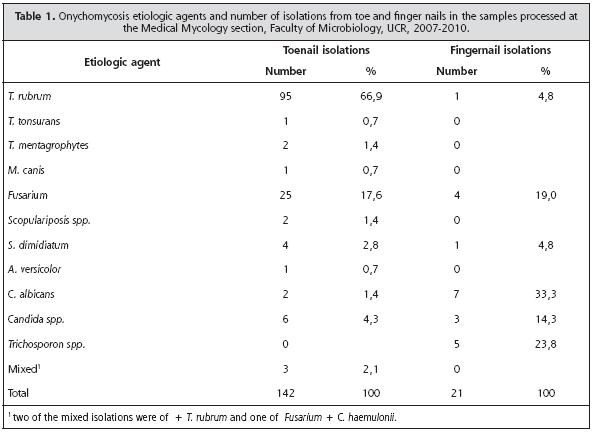
142 (51.6%) samples 147 isolations were obtained. Of these, 103 (70.1%)
were dermatophytes, 9 (6.1%) were yeasts,
and 35 (23.8%) were
non-dermatophyte filamentous fungi (Table 1).
Among the
33 finger onychomycoses,
7 (21.2%) were from males and 26 (78.8%) from females.The
age distribution is shown in Figure 1.Thirty samples (90.9%) had a
positive
direct examination. In 12 samples (36.4%) it was impossible to
determine an
etiologic agent and in 21 (63.6%) there was a positive isolation. Of
these, 1
(4.7%) was a dermatophyte, 10 (47.6%) were
yeasts,
and 10 (47.6%) were non-dermatophyte
filamentous
fungi (Table 1).
Discussion
The
majority of the cases that are received by our
laboratory are due to onychomycoses as has
been
reported by other studies.14-16 Pathologies similar to this
infection include pachyonychia, ungual
dyschromia, acquired dystrophies, or
changes due to
diseases such as pityriasis rubra
and psoriasis,17 which could
explain the onychodystrophies that some
patients present.
Nowadays, onychomycoses
represent a public health problem because of their interpersonal
transmission,
their high prevalence among the population,16 the difficulty
of
their treatment3 and because they are favored by modern
activities
such as exercising in gymnasiums, the use of public pools and baths,
the
easiness of travel and the use of occlusive shoes.9,16-18
Moreover,
it has been reported that the global incidence of this condition is
rising as
well as the factors that facilitate its development, such as diabetes,
vascular
problems and nail trauma.16
As it has
been reported in the literature,14,16,19
in our laboratory some samples for
which a positive direct examination was obtained, it was impossible to
isolate
an etiologic agent. This could be due to the fact that the sample was
not
representative because there is a higher possibility that the fungus is
alive
in the proximal area of the nail where access for sample collection is
more
difficult. Moreover, some patients apply to themselves topic treatments
or take
antimycotics that impair the isolation of
the fungal
agent. For this, it is indispensable to recommend the patient not to
apply or
take antimycotic medication before the
sample
collection.
It is
important to know the epidemiology of onychomycoses
in a country because it can vary between
different geographic areas in terms of their frequency by gender, age
and
etiologic agent.15 In this study, a higher amount of cases
were seen
among women as has been described in other countries.16 This
could
be due to the fact that in many countries women are more frequently
employed in
domestic labor,20 which favors
the
maceration of the skin, a predisposing factor for finger onychomycoses.
In turn, it could also be due to the fact that women are in general
more aware
of their health, their physical appearance and have easier access to
medical
consultation, factors that could make the statistics not reflect the
real
situation regarding onychomycoses.20,21
With
regards to the age of the patients, a higher
number of consultations and diagnoses of onychomycosis
was registered for patients between 40-60 years of age, which agrees
with what
has been reported in other latitudes.1,15,16,20 Even though
children
and adolescents suffer onychomycoses, it
is expected
that most cases will be observed among adults because of factors such
as a
slower growth of the nail, the presence of microtraumata
due to occlusive shoes or sport (onychomycoses
among
barefooted people are rare), 15as well ashigher
work activity, venous insufficiency and even a higher exposure to the
fungus.16
Also, the low frequency among children could be due to the structure of
the ungual plaque, a lack of accumulated
traumata, fast ungual growth and the
subsequent elimination of the fungus.16,20
The reduction in cases after 60 years of age could be due to low
motivation to
consult for a problem that many consider to be aesthetic or even to
follow a
treatment regime.9 However, if we consider the possible
complications that could arise in elderly patients, these conditions
should not
be left without a proper diagnosis and treatment.10,12
T. rubrum was
the most common etiologic agent isolated from the toenails. This fungus
is the
most commonly reported in many countries,11,15,21,22
possibly due to
its anthropophilic character, which is
favored by
modern activities such as those described previously.
Among the
non-dermatophyte
filamentous fungi, Fusarium spp.was the most common agent in toenails, while
Trichosporon spp. was the most
common in
fingernails. In European countries, non-dermatophyte
filamentous fungi represent 1.5-6% of all onychomycosis
cases,23,24 while in countries
such as
Onychomycoses
caused by Fusarium spp. do
not respond
to treatment with fluconazole, and because
of this
these infections must be treated with terbinafine
and
itraconazole with satisfying results,7 as well as with ciclopirox
in spray after a total or partial elimination of the nail with 40% urea.12
In this
study, we were able to isolate Scopulariopsis
brevicaulis
and Aspergillus versicolor
from toenails. For the treatment of these cases oral terbinafine
or itraconazole, as well as the partial or
total
extraction of the nail with ciclopirox as
an ointment
or a spray, bifonazole or terbinafine
as nail cream.6,7,25
Regarding Scytalidium
dimidiatum, even though it was isolated
only in a
few cases, its identification is relevant because it is generally
considered
incurable,8 requiring chemical
ablation of
the nail along with ciclopirox or 5% amorolfine. For this fungus, voriconazole
has been tested in vitro, showing a low minimal inhibitory
concentration; hence
its use in these infections should be considered.8
In
fingernails, C. albicans
was the most commonly isolated species. Trichosporon
spp. was only isolated from fingernails. This fungus has been reported
in other
countries, although its role as a causative agent is disputable and it
could
even be considered as a invader secondary
to damage to
the nail.11
References
1. Burzykowski T, Molenberghs G, Abeck D, Haneke E, Hay R, Katsambas A, et al. High prevalence of foot diseases in Europe: results of the Achilles Project. Mycoses 2003; 46:496-505. [ Links ]
2. Lagana FJ. Curing onychomycosis: understanding the multitude of variables. Clin Podiatr Med Surg 2004; 21:555-564. [ Links ]
3. Arrese JE, Piérard-Franchimont C, Piérard GE.Fatal hyalohyphomycosis following onychomycosis in an immunocompromised patient.(Extraordinary case report). Am J Dermatopathol 1996; 18:196-198. [ Links ]
4. Chadeganipour M, Nilipour S, Ahmadi G. Study of onychomycosis in Isfahan, Iran. Mycoses 2009; 53: 153-157. [ Links ]
5. Neji S, Makni F, Cheikhrouhou F, Sellami A, Sellami H, Marreckchi S, et al. Epidemiology of dermatophytosis in Sfax, Tunisia. Mycoses 2009; 52: 534-538. [ Links ]
6. Souza LKH, Fernandes OFL, Passos S, Costa CR, Lemos JA, Silva MRR. Epidemiological and mycological data of onychomycosis in Goiania, Brazil. Mycoses 2009; 53: 68-71. [ Links ]
7. Carrillo-Muñoz AJ, Tur-Tur C, Hernández-Molina JM, Santos P, Cárdenas D, Guisiano G. Antifúngicos disponibles para el tratamiento de las micosis ungueales. Rev Iberoam Mycol 2010; 27: 49-56. [ Links ]
8. Drake LA, Sher RK, Smith EB, Faich GA, Smith SL, Hong JJ, et al. Effect of onychomycosis on quality of life.J Am Acad Derm 1998; 38: 702-704. [ Links ]
9. Svejgaard EL, Nilsson J. Onychomycosis in Denmark: prevalence of fungal nail infection in general practice. Mycoses 2004; 47:131-135. [ Links ]
10. Roberts DT, Taylor WD, Boyle J. Guidelines for treatment of onychomycosis. Br J Dermatol 2003;148: 402-410. [ Links ]
11. Bourgenois GP, Cafardi JA, Sellheyer K, Andea AA.Disseminated Fusarium originating from toenail paronychia in a neutropenic patient.Cutis 2010; 85: 191-194. [ Links ]
12. Salas-Campos I, Gross-Martínez N, Carrillo-Dover P. Micosis superficiales diagnosticadas en el laboratorio de micología médica de la Universidad de Costa Rica. Rev Costarricense de Ciencias Médicas 2007; 28(1,2): 29-35. [ Links ]
13. Salas-Campos I, Gross-Martínez N, Carrillo-Dover P. Onicomicosis por hongos fuliginosos. Acta Médica Costarricense 2009, 51(4):241-244. [ Links ]
14. Gianni C, Cerri A, Crosti C. Non-dermatophyticonychomycosis. An understimated entity?A study of 51 cases. Mycoses 2000; 43:29-33. [ Links ]
15. Gupta AK, Gregurek-Novak T, Konnikov N, Lynde CW, Hofstader S, Summerbell RC. Itraconazole and terbinafine treatment of some nondermatophyte molds causing onychomycosis of the toes and a review of the literature. J Cut Med Surg 2001; 5:206-210. [ Links ]
16. Lacroix C, Feuilhade de Chauvin M. In vitro activity of amphotericin B, itraconazole, voriconazole, posaconazole, caspofungin and terbinafine against Scytalidiumdimidiatum and Scytalidiumhyalinumclinical isolates. J Antimicrobial Chemotherapy 2008; 61:835-837. [ Links ]
17. Hashemi SJ, Gerami M, Zibafar E, Daei M, Moazeni M, Nasrollahi A. Onychomycosis in Tehran: mycological study of 504 patients. Mycoses 2009; 53:251-255. [ Links ]
18. Padilla-Desgarennes MC. Diagnóstico diferencial en onicomicosis. Pfizer SA de CV. México, 2000. [ Links ]
19. Midgley G, Moore MK. Onychomycosis. Rev Iberoam Micol 1998; 15:113-117. [ Links ]
20. Ogasawara Y, Hiruma M, Muto M, Ogawa H. Clinical and mycological study of occult tinea pedis and tinea unguium in dermatological patients from Tokyo. Mycoses 2003; 46:114-118. [ Links ]
21. Bokhari MA, Hussain I, Jahangir M, Haroon TS, Aman S. Onychomycosis in Lahore, Pakistan. Inter J Dermatol 1999; 38: 591-595. [ Links ]
22. Koussidou T, Devliotou DD, Karakatsanis G, Minas A, Mourellou O, Samara K. Onychomycosis in Northern Greece during 1994-1998. Mycoses 2000; 37:29-37. [ Links ]
23. Barua P, Barua S, Borkakoty B, Mahanta J. Onychomycosis by Scytalidiumdimidiatum in green tea leaf pluckers: report of two cases. Mycopathologia 2007; 164:193-195. [ Links ]
24. De Magalhaes-Lima K, Machado-Barbosa de Castro CM, Fonseca Nogueira CII, Carvahaes de Oliveira J, Delgado M, Sette de Melo RR. Hongos filamentosos no dermatofitos: onicomicosis en cuatro pacientes infectados con el virus de la inmunodeficiencia humana. Rev Iberom Micol 2008; 25:49-45. [ Links ]
25. Garg A, Venkateshk V, Singh M, Pathak KP, Kaushal GP, Agrawal SK. Onychomycosis in central India: a clinicoetiologic correlation. Int J Dermatol 2004; 43:498-502. [ Links ]


{kind=link}
{kind=link}