










Servicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkActa Médica Costarricense
versión On-line ISSN 0001-6002versión impresa ISSN 0001-6012
Acta méd. costarric vol.54 no.2 San José abr./jun. 2012
Original
El polimorfismo
inserción/deleción del gen de la enzima convertidora de
angiotensina y su asociación con algunas complicaciones en pacientes
con
diabetes mellitus tipo 2
(Angiotensin
Converting Enzyme Insertion/Deletion Polymorphism and its Association
with
Complications in Patients with type 2 Diabetes Mellitus)
Diego Moya-Zeledón, Juan José Madrigal-Sánchez, Lizbeth
Salazar-Sánchez
Translated by: Javier Estrada Zeledón
Abstract
Background:
Diabetes
mellitus is a disease with serious repercussions on the Costa Rican
population
and it predisposes patients to diverse complications. The exact origin
of these
complications is not known; it has been suggested that certain
polymorphisms
are strongly associated with the appearance of some of them.
Aim: To
determine if there is a relation between complications from diabetes
and the
insertion/deletion polymorphism of the angiotensin
converting enzyme.
Methods: This
investigation included 225 subjects. 109 were cases and 116 control
subjects. A
blood sample was taken from each participant and fibrinogen levels were
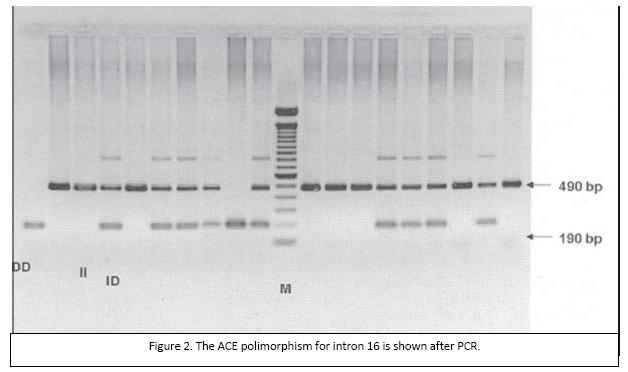
measured; also, using a polymerase chain reaction of the intron
16 of the angiotensin converting enzyme
gene, the
insertion/deletion mutation of the angiotensin
converting
enzyme was studied. Then, the results were compared to the presence of
diabetes
or its complications.
Results: A
greater number of controls were found to have insertion/deletion
polymorphism,
however this was not considered statistically significant. In the case
group,
none of the polymorphisms showed a dominant behavior. D/D was
associated with
high levels of fibrinogen.
Conclusion: No
strong association was found between the polymorphisms of the Angiotensin converting enzyme and suffering from
Diabetes
mellitus type
Keywords: Diabetes
mellitus, angiotensin converting enzyme,
polymorphism, PCR
Diabetes
mellitus (DM) is a set of metabolic disorders
that share hyperglycemia as a common phenotype. 1 Different types of
diabetes
exist, and they are related to a complex interaction between genes,
environment
and lifestyles. Factors contributing to hyperglycemia may be due to
decreased
or absent secretion of insulin, decreased glucose consumption or
increased
glucose production. 2.3 The lack of glucose metabolism regulation
causes
several pathophysiological changes in
multiple
organs; most common complications include dyslipidemia,
nephropathy and vascular abnormalities. 4
Nowadays,
there are more than 143 million people with
DM worldwide 5, representing one of the major health problems worldwide
as it
implies high costs for any country. In Costa Rica it is estimated that
by 1998
the self-reported prevalence of DM was 4.8% for people over 20
years-old, by
2006 it was estimated that the percentage of diabetic patients went up
to 5.3%
in this population, 1 showing the importance that this disease has
claimed
along time for health authorities in Costa Rica. 6
According
to the CARMEN survey 7 for the diabetic
population, gender percentages indicate that the prevalence is higher
in women
(3.4%) than men (2.2%), the average age at death is 65, and also it is
known
that the prevalence of DM is lower in rural areas, both inside and
outside the Costarican Central Valley. 8
The urban area showed a 10,2% prevalence
both in and out from the Central Valley. 8
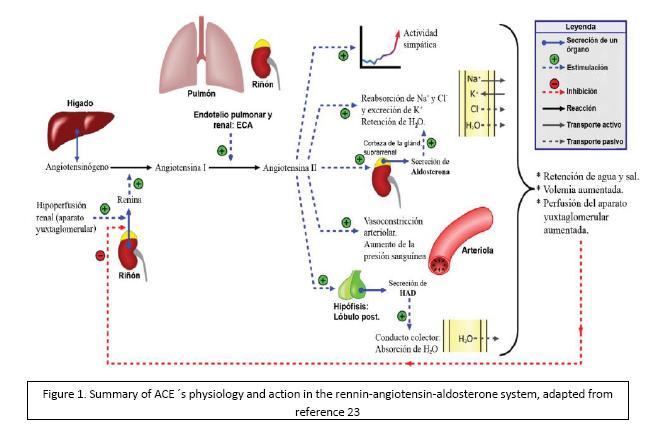
Angiotensin converting enzyme (ACE)
Materials and Methods
A
population of 225 individuals was studied, of whom
there were 109 cases and 116 controls, the case group were those
diabetic
patients who were treated in areas covered by the Basic Teams for
Comprehensive
Health Care (Equipo Básico
de Atención Integral de Salud,
EBAIS), within the comprehensive health care program of the Costarican
Social Security Fund (Caja Costarricense
del Seguro Social, CCSS)-University of
Costa Rica
agreement, from March 2007 to July 2008. The control group
were those non-diabetic individuals willing to participate
freely in the
study.
Each
individual had to sign an informed consent form
(project number 807-A5-311, approved by the document VI-8163-2008) to
be
included in the investigation as provided by the Bioethics Committee of
the
Universidad de Costa Rica´s Research
Vice-Rectory.
Because of
a coincidence in terms of patients studied,
in both case and control groups there was a clear majority of women; 86
(74%)
of control individuals, and 73 (67%) of the case individuals were women.
Studies
performed
Sample
gathering and stability:
Two peripheral blood samples were obtained from each patient, one with
EDTA as
an anticoagulant and the other one with citrate. This was kept
refrigerated
since it was drawn, and plasma was separated from blood cells as soon
as
possible.
Molecular-genetic
analysis:
DNA isolation was made by the standard precipitation method with NaCl, as described by Miller et al. 13 The I/D
mutation
study for the ACE gene was performed through the polymerase chain
reaction
(PCR) of intron
Coagulation
analysis:
plasma was frozen to -70° C to be analyzed in a two month-maximum time
lapse, values of plasma fibrinogen (FGO) were obtained by the method
described
by Clauss in 1957 15.
Data
analysis: The
information obtained by interviews and laboratory tests was digitized
and data
analysis was made using the Epi-Info6d software; a binomial logistic
model was
also used, using the version 13.0 SPSS software (SPSS Inc,
Results
We
compared the number of individuals in the study who
suffered strokes, dyslipidemia,
nephropathy and
ischemic heart disease in both groups without obtaining a significant
difference between the number of cases and number of controls who
suffered such
pathologies. In the case of high blood pressure (hypertension), there
was a
significant difference, according to what was expected. (Table 1)
As for the
ACE I/D gene polymorphism, there was a
greater number of controls with the ACE I/D polymorphism, without being
significant. In the case group, no polymorphism showed a dominant
behavior,
with almost the same number of individuals for each polymorphism.
We looked
for the relationship between having or not a
stroke and the ACE polymorphism for each individual, without a
significant
difference between any of the 3 polymorphisms for this disease. A
similar behavior
was observed when looking for a relationship between ACE polymorphism
and the
presence of ischemic heart disease, dyslipidemia,
hypertension and nephropathy.
When
performing a χ2
comparing the variable FGO with
D/D polymorphism, a p= 0.026 was obtained, which indicates that the D/D
polymorphism is associated with abnormal levels of FGO, so that the D/D
polymorphism is apparently associated with some complications of
diabetes
(Table 2), as it
is a confusing variable.
The
polymorphism allelic frequencies for the controls
met the Hardy-Weinberg equilibrium. The ACE I/D does not meet the
Hardy-Weinberg equilibrium (χ2 = 10,36; df= 2; p =
0.005).
Finally,
it was seen that among the 116 individuals of
the control group, 68% had normal plasma FGO levels while 29% of this
group had
altered plasma FGO levels. For the case group 72% out of 109
individuals had
altered plasma FGO levels, while 22% had normal levels.
Discussion
As for the
ACE polymorphism and its association with cerebrovascular
disease, this research shows no association
with each other and data indicate that the endothelial damage and prothrombotic state present in diabetes must
have other
factors besides this gene. Similar results can be found in the
literature,
giving much greater weight to this finding 16.
The
literature indicates that the sequence of the I
allele in the ACE I/D, is similar to that of a
"silencer", this could explain the association of the D allele with
high plasma levels of ACE, producing hypertension (HTN); 17 -19 the
study
population slightly showed this behavior without being statistically
significant.
The
presence or absence of hypertension was not
significantly different when compared with the 3 studied polymorphisms;
however, by the applied logistic regression model, the D/D polymorphism
is
related to a predisposition to develop diabetes, but this variable can
barely
explain 3,58% of the variability, so that the important etiology of DM
depends
on other factors. One idea that emerges is that perhaps the D/D
polymorphism is
a confounding variable when studying the I/D ACE polymorphism, this
means that
possibly there is another variable not taken into account, besides I/D
ACE
polymorphism that really influences suffering or not from DM and its
complications; then the fact of having or not DM and its complications
is
associated with this factor, which was not considered in this study.
This
finding may also be due to sample size, which in this case is small for
genetic
research purposes. Also, it could be because the study population does
not have
a true relationship between hypertension and the ACE polymorphism,
which is
shown in the results; Mondry et al 20
obtained
similar results with a larger sample size, so that this supports the
idea that
there is no relationship between hypertension and ACE in the study
population.
Both nephropathy, dyslipidemia,
as in ischemic heart disease showed no tendencies towards any of the
studied
polymorphisms. In Costa Rica, specifically in the Central Valley, a
study has
been made, revealing the genetic origins of the population 21 and
another one
that investigates conditions according to gene origins, showing that
the more
the Western-African heritage a person has, the greater the risk of
myocardial
infarction and hypertension, while the more the indigenous heritage,
the
greater the risk of metabolic syndrome. 22 However, there were no Costa
Rican
reports found about ACE I/D polymorphisms and their relationship with
the
complications studied in this research. Reports were found from Asian,
European
and
The
allelic frequencies of the ACE I/D polymorphism
for the cases group do not meet the balance proposed by the
Hardy-Weinberg equilibrium.
This is probably due to sample size which is not suitable for this type
of
analysis (n = 225), coupled with the fact that ideally the analysis is
applied
to samples in which different generations are included, so that the mutation´s behavior could be compared throughout
generations. Further research is suggested to increase the sample size
and
achieve statistically significant results.
For an
inference about the ACE gene polymorphism on
the Costa Rican population, it is necessary a bigger study in which an
adequate
sampling is done, taking into account epidemiological parameters; once
an
adequate number is obtained and an appropriate selection of each individual´s original location is made, the
variability of the polymorphism in the Costa Rican population should be
established, and then an inference could be made about the relationship
of the
ACE gene in certain pathologies in the Costa Rican population.
Levels of
FGO in the diabetic population are known to
be generally changed, 17 this was important when performing data
analysis and
obtaining an apparent association of the D/D polymorphism with some of
the
studied complications. When analyzing this background detail it was
concluded
that individuals with the D/D polymorphism are linked to altered FGO
values,
this is why FGO is identified as the cause of the associated
complications,
subtracting the effect of the FGO variable,
the real
effect of the polymorphism meant no significant value.
Conflicts
of interest:
none of the authors reported conflicts of interest performing this
research.
1. Ayala N, Fernández A, León M, Villegas O. Control de la diabetes en las personas atendidas en la Caja Costarricense de Seguro Social. http://www.ccss.sa.cr/html/organizacion/gestion/gerencias/administrativa/dcss/archivos/estudios_realizados/04.pdf. [ Links ]
2. Rodríguez Weber F, Sáenz Tapia G. Obesidad, hipertensión arterial y DM: ¿Puntos de partida o finales de un mismo problema? Med Int Mex 2008; 24:342-5 [ Links ]
3. Beckham J, Creager M, Libby P. Diabetes and Atherosclerosis Epidemiology, Pathophysiology, and Management. JAMA 2002; 287: 2570-2581 [ Links ]
4. Kasper D, Braunwald E, Fauci A. Harrison: Principios de Medicina Interna. 16ed Mc Graw-Hill, México. 2006: 2367-2369 [ Links ]
5. Roselló-Araya M, Araúz-Hernández A, Padilla-Vargas G, Morice- Trejos A. Prevalencia de diabetes Mellitus auto-reportada en Costa Rica, 1998. Act méd costarric 2004; 4:190-195. [ Links ]
6. Brenes-Camacho G, Rosero-BixbyL. Diabetes mellitus en adultos mayores costarricenses. Pob Salud Mesoam, 2007;5 Recuperado el 20 de junio del 2009 de http://www.ccp.ucr.ac.cr/creles/cientif.htm. [ Links ]
7. Organización Panamericana de Salud (OPS). Red Panamericana: Conjunto de Acciones para la Reducción Multifactorial de las Enfermedades No transmisibles (CARMEN). [serie en internet]. Recuperado el 20 de junio del 2009 de http://www.paho.org/Spanish/AD/DPC/NC/carmen-info.htm. [ Links ]
8. Ministerio de salud. Desigualdades de salud en Costa Rica. Serie análisis de situación de salud 2003, No 8: 25 [ Links ]
9. Mauer K, Exaire JE, Escalante B. Importancia de la ECA en la circulación coronaria. Arch cardiol mex 2001;71:278-285 [ Links ]
10. Eisenmann J C, Sarzynski1 M A, Glenn K, et al. ACE I/D genotype, adiposity, and blood pressure in children. Cardiovasc Diabet 2009 ; 8:14 [ Links ]
11. Coto E . Polimorfismos del gen de la ECA y enfermedad cardiovascular. Nefrol 2001; 21:67-9 [ Links ]
12. Marre M, Jeunemaitre X, Gallois Y. Contribution of Genetic Polymorphism in the Renin–Angiotensin System to the Development of Renal Complications in Insulin-dependent Diabetes. J. Clin Invest 1997; 99:1585–1595 [ Links ]
13. Miller SA, Dykes DD, Polesky HF. A simple salting out procedure for extracting DNA from human nucleated cells. Nucl Acids Res 1998 ; 16:1215 [ Links ]
14. Rigat B, Hubert C; alhenc-Gelas F, Cambien F, Corvol P, Soubrier. Insertion/deletion polymorphism in the angiotensin I-converting enzyme gene accounting for half the variance of serum enzyme levels. J Clin Invest 1990; 1343-1346 [ Links ]
15. Sáenz G. Hematología analítica, Tomo II. 5 Ed, EDNASSS, Costa Rica, 2005: 9-16 [ Links ]
16. Catto A, Carter A, Barret J, Stickland m, Bamford J, Davies A, Grant P. Angiotensin-converting enzyme Insertion/Deletion Polymorphism and cerebrovascular disease stroke. JAMA 1996; 27:435-440 [ Links ]
17. Carluccio M, Soccio M, De Caterina R. Aspects of gene polymorphisms in cardiovascular disease: The renin-angiotensin system. Eur J Clin Invest 2001; 31:476-488 [ Links ]
18. Ganong W. Fisiología Médica. 19ed Editorial H Manual Moderno, México. 2004: 871 [ Links ]
19. Niu T, Chen X, Xu X. ACE gene insertion/deletion polymorphism and cardiovascular disease. Drugs 2002; 62:977-993 [ Links ]
20. Mondry A, Loh M, Liu P, Zhu A, Nagel M. Polymorphisms of the Insertion/deletion ACE and M235T AGT genes and hypertension: surprising new findings and meta-analysis of data. BMC nephrology 2005; 6:1 [ Links ]
21. Segura-Wang, M, Raventós H, Escamilla M, Barrantes R. Assessment of Genetic Ancestry and Population Substructure in Costa Rica by Analysis of Individuals with a Familial History of Mental Disorder. Ann Hum Genet. 2010, 74; 516–524 [ Links ]
22. Ruiz-Narváez EA, Bare L, Arellano A, Catanese J, Campos H. West African and Amerindian ancestry and risk of myocardial infarction and metabolic syndrome in the Central Valley population of Costa Rica. Hum Genet. 2010, 127; 629-38 [ Links ]
23. Wikimedia Commons. Archivo: Sistema Renina-Angiotensina- Aldosterona.png. Depósito de contenido libre Wikimedia Commons. Recuperado el 2 de febrero de 2011 de: http://upload.wikimedia.org/wikipedia/commons/4/4b/Sistema_ Renina-Angiotensina-aldosterona.png. [ Links ]
24. Lizaraso F, Rivara G, Torres E, Fujita R. Presencia del genotipo D/D del gen de enzima convertidora de angiotensina y del genotipo 235T del gen de angiotensinógeno como factores de riesgo para sumir un evento coronario agudo. Rev peru cardiol 2002; 28: Recuperado el 23 de febrero de 2011 de http://sisbib. unmsm.edu.pe/bvrevistas/cardiologia/v28_n1/presen_geno.htm. [ Links ]
Fecha
recibido: 29
de marzo de 2011 Fecha aceptado: 26 de enero de 2012


{kind=link}
{kind=link}
{kind=link}
{kind=link}